from: A Midwestern Doctor from The Forgotten Side of Medicine <amidwesterndoctor@substack.com>
reply-to: A Midwestern Doctor from The Forgotten Side of Medicine <reply+2go2jb&doii8&&9ecf4cb0a4b742ff0361bedfb060a6128723758761d1ff353a6538964e0c8141@mg1.substack.com>
to: fchase@gmail.com
date: Sep 15, 2024, 7:57 PM
subject: DMSO Could Save Millions From Brain and Spinal Injury
mailing list: amidwesterndoctor@substack.com Filter messages from this mailing list
mailed-by: mg1.substack.com
signed-by: mg1.substack.com
security: Standard encryption (TLS) Learn more
: Important mainly because it was sent directly to you.
This page constitutes commentary, based on Fair Use, on a
thought-provoking and insightful document.
You are encouraged to see the document in its
original context unless you are interested in this Commentary Markup by Frederick N. Chase.
The markup is only via
i) emphasis (yellow highlight, red, bold, underline, or
font size),
ii) [pink bracketed commentary],
iii) hypertext linking of a term or statement to a
web page believed to offer quick uncontroversial augmentation and
iv) omission (elision) of material – indicated by a series of dots somewhat
proportional to the amount of original material elided.
This page is part of the homeplace web portal. Homeplace is advertisement-free and not for
profit.
|
Keyword |
Reference |
|
DMSO |
398 |
|
Dimethyl sulfoxide |
5 |
|
hemorrhagic strokes |
3 |
|
ischemic strokes |
7 |
DMSO Could Save Millions From Brain and Spinal Injury
The decades of evidence showing DMSO revolutionizes the care of many "untreatable" circulatory and neurologic conditions.
Sep 15, 2024
∙ Paid
364
62
Story at a Glance:
•DMSO is a remarkably safe chemical that protects cells from otherwise fatal stressors (e.g., freezing, burning, shockwaves, ischemia). Since the heart, brain, and spinal cord are particularly vulnerable to injury, DMSO can produce miraculous results for those conditions.
•The usage of DMSO
completely transforms the management of strokes (including brain bleeds), heart
attacks, and spinal cord injuries. As I will show here, had the FDA not
sabotaged DMSO’s adoption, in addition to countless lives being saved, millions
could have been protected from a lifetime of disability or paralysis.
•DMSO has many other remarkable properties. For example, it stabilizes
proteins, and thus treats many challenging protein disorders (e.g., amyloidosis
and numerous genetic disorders).
•Many conditions DMSO treats are typically considered to be incurable. In this article, I will focus on DMSO’s remarkable utility for the conditions that respond best to intravenous DMSO (e.g., a variety of circulatory disorders like varicose veins or Raynaud’s) and complex neurological disorders (e.g., Down’s Syndrome, Developmental Delay, ALS, Alzheimer’s, Parkinson’s), along with how to administer IV DMSO and DMSO stroke protocols.
If I were stranded on a
desert island or knew the world was ending and I could only bring a few
therapies with me, one of them, without a doubt, would be DMSO. This is
because:
•It treats a wide range of severe illnesses which are often otherwise incurable
and frequently fatal or lead to a lifetime of permanent disability.
•It effectively treats acute injuries and rehabilitates chronic musculoskeletal
disorders (e.g., arthritis). Because of this, it’s
one of the best “pain medicines” out there and has allowed many to get
their lives back.
•It has a variety of unique properties that open up a completely different
dimension to how medicine can be practiced.
•It is one of the safest medically active
substances in existence.
Remarkably, in the 1960s, this was recognized and DMSO took the nation by storm (e.g., people everywhere were clamoring for it, gas stations would often advertise they sold it, and tens of thousands of research studies were conducted by enthusiastic scientists around the globe). Now however, outside of it being a laboratory chemical or an alternative therapy some people use for joint pain, few are even aware of DMSO’s existence.
This was due to the FDA waging a multi-decade long war against DMSO (despite widespread outcry from Congress and the public), which I believe was arguably the worst thing the FDA has ever done to the country.
Since I am uniquely positioned to present many of the forgotten sides of medicine to the public, I’ve long felt the DMSO story needs to be told. Simultaneously however, since there is a wealth of data on this topic, I wanted to ensure I honored the importance of this subject and accurately present it. For this reason, I’ve spent the last three months reading and arranging thousands of pages of literature. Since there is so much to say on this topic, this series will be broken into a few parts. In the first installment, I will cover the key properties of DMSO and the challenging conditions where it provides the most profound benefits.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber. To show how others have benefitted from this newsletter, click here!
Subscribed
What is DMSO?
Dimethyl sulfoxide, as the name implies, is comprised of two methyl groups and an oxygen atom bonded to sulfur. This simple chemical and its breakdown products exist in nature (e.g., they can be found in small amounts in milk, tomatoes, tea, coffee, beer clams, and cooked corn, while the salty smell of the ocean is, in part, due to microalgae near the surface creating dimethyl sulfoxide—some of which also makes it into the rain).
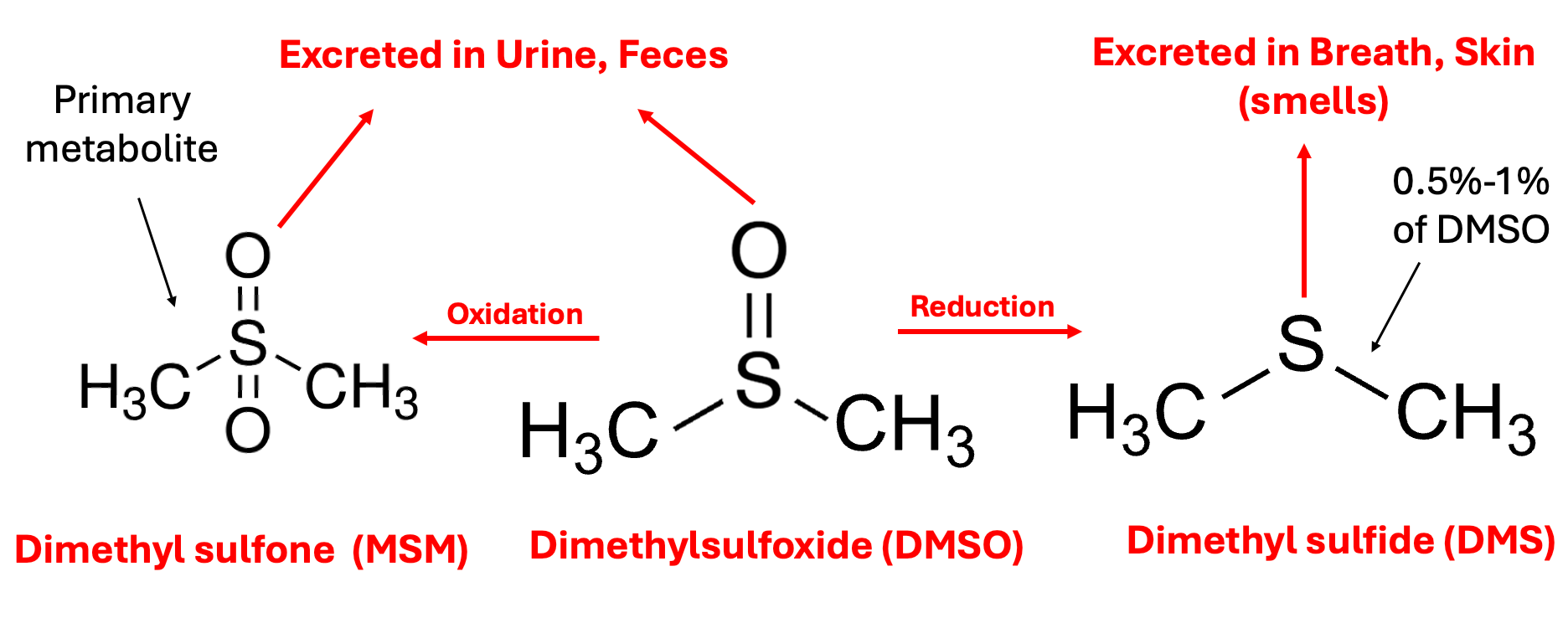
In the body, DMSO is then oxidized or reduced, with the oxidized form (more commonly known by the name methylsulfonylmethanethe or MSM—a common joint healing supplement) being the primary fate of it, while the reduced form DMS (which naturally exists in trace amounts in the body) is the more notorious metabolite because it is responsible for DMSO’s characteristic “side effect,” a distinctive garlic or clam-like odor (or taste) that is excreted through the mouth and skin which certain individuals have difficulty tolerating (and forcing certain longterm DMSO users to creatively arrange their social life). This effect typically lasts a few hours, but in certain cases can last up to 72 hours, and appears to be reflective of the overall health of the body (since as people detox, their DMSO odor decreases).
Note: one school of thought in integrative medicine (e.g., Dr. Mercola is a strong proponent of this model) argues that insufficient oxidation, which leads to a build-up of reduced molecules in the body (termed reductive stress) is a root cause of many illnesses (e.g., the mitochondria cannot function properly if the electron transport chain is reduced). The susceptibility to the DMSO odor is one of the best illustrations I have found of this model, particularly since there are many reports showing that concurrently taking chlorine dioxide (an oxidizing agent) eliminates it (as does a user’s overall health improving over time). Likewise, some DMSO users and one study have found that when DMSO was taken at the same time as alcohol (another oxidizing agent), the odor was reduced, whereas when alcohol was given an hour after DMSO, the opposite occurred (which touches upon the fact DMSO can sometimes cause excessive drowsiness if combined with a sedative).
Due to its relatively small
size, having both a polar and non-polar half, being able to form hydrogen bonds
slightly stronger than those found between water molecules, and not releasing
protons, DMSO has two remarkable properties:
•It acts as a
near-universal solvent (e.g., it interacts with a vast range
of biomolecules and can easily mix with any concentration of water).
•It’s able to pass through biological membranes without damaging them (something to my knowledge, nothing else can do).
Because of this, DMSO will rapidly enter the body (including the brain) regardless of its route of administration (e.g., within 5 minutes after going on the skin it can be found in the blood, and within an hour it can be found within the bones), but simultaneously does not accumulate within the body after prolonged use (and virtually none remains a week after administration).
Note: in one study of rats, radio-labeled DMSO was found to enter all tissues of the body within 30 minutes (with the highest levels seen in the plasma, kidney, spleen, lung, heart, and testes and the lowest in the lens of the eye), with DMSO levels declining to minimal levels after 24 hours, while another study found orally administered DMSO reached a peak blood level in 4 hours and was undetectable after 120 hours, while MSM appeared in the blood after 48 hours and disappeared after 400 hours (with another human study finding similar results).
DMSO in turn, has an almost endless amount of uses as it can be applied in almost any manner (e.g., it is frequently applied through the skin—although less is absorbed in this manner than the other routes of administration). Almost any drug or substance can be combined with it and administered through the skin (e.g., steroids, NSAIDs, numerous antibiotics or antivirals, glucose, vitamin C, hydrogen peroxide, or chlorine dioxide). In many cases, the effect of those drugs is enhanced, and simultaneously, their toxicity is reduced (although, in some cases, the toxicity increases).
Note: DMSO is less effective at bringing larger molecules into the body (e.g., it had been hoped it could be mixed with insulin so diabetics could have a way to bypass the need for injecting insulin—but this didn’t work).
Cellular Protection
DMSO’s ability to spread throughout the body (including into the brain) initially seems concerning—however rather than be toxic to cells, DMSO heals them and protects them from damage and a wide range of otherwise lethal stressors. Since DMSO does not expand when it freezes (at 65.4°F), this property (and the fact that a 66% DMSO 33% water mixture freezes at -99.4°F), has made it a revolutionary substance for preserving frozen cells (e.g., stem cells). In contrast, very few other substances exist that cells can tolerate such a high concentration of.
Note: since some of the information I need to present here is a bit technical for those wanting more references, if you find some of the information is too dense, skip over it. Additionally, I need to acknowledge many of these experiments were cruel and go against my own values of supporting animal welfare.
DMSO, in turn, has been shown to:
•Protect tissue from dying when its blood supply is cut off (e.g., in skin flaps, in the kidneys [replicated here], in the small intestine, in the liver, or in the heart—particularly when hydrogen peroxide is given concurrently as an oxygen donor), prevent a reperfusion injury when its blood flow is restored, prevent the formation of clots when blood flow is restored (e.g., in mesenteric veins), reduce the amount of permanently damaged tissue following a myocardial infarction and maintain the heart’s ability to circulate blood when its blood supply is cut off.
•Prevent heart damage caused by dietary copper deficiency and kidney failure caused by toxic mercury exposure.
•Increase the production of
ATP in cells (e.g., minute concentrations of DMSO have been shown to
increase metabolism by shunting metabolites from glycolysis to the
mitochondrial Krebs cycle), which likely both accounts for some of DMSO’s
protective effects and its anticancer effects.
•Prevent a rapid
influx of calcium or sodium ions, a process which frequently
occurs when a cell’s viability is threatened (and then results in the death of
the cell).
•Prevent asphyxiation from being lethal (e.g., one study put rats into a pure nitrogen environment for 210 seconds, and found that 90% who received DMSO in advance survived compared to 15% of those that received saline).
•Protect cells from being destroyed by sonic disruption via an ultrasonic vibrator (with 78% of cells receiving 10% DMSO surviving compared to 13% of controls).
•Save the fingers of individuals with severe frostbite that would otherwise require amputation. DMSO has also been shown to protect cells from freezing damage, and to protect rabbit ears and thighs from being damaged by frostbite induced by immersion in a -42°C bath.
•Treat a variety of burns without being prone to producing infections (e.g., a 1985 study by Russian burn specialists, in adolescents, found DMSO was superior to the other treatment options [nitrofurazone, trimecaine, and monomycin]). This includes severe acid skin burns (along with preventing their progress), and both acidic and alkaline burns that erode the esophagus (e.g., by inhibiting the destructive inflammatory response following those esophageal burns).
Finally, a study of 1371 patients with skin disorders (including 173 patients with second or third-degree burns on the hands, feet, and legs) who received a topical DMSO spray approximately three times a week found that 95.04% had a complete recovery, with the majority of the remaining 4.96% being due to premature cessation of DMSO or the patient no longer being under observation.
There are also cases of severe burns that within minutes stopped hurting (a major problem with burns), didn’t blister, and recovered completely. One of the most extraordinary ones (reported by William Campbell Douglass) involved six year old girl who’d slipped her index finger in a light socket for a prolonged period, after which it was cooked through and burned ash white at the tip. Within 30 minutes Douglass got the finger into a full-strength DMSO bath, and after 20 minutes, the searing pain had disappeared, the next day the finger turned pink, and then rather than be lost, fully recovered.
Note: patients have also reported DMSO relieves sunburns in 10-30 minutes.
•Protect cells from being damaged by (often otherwise fatal) radiation. For example, numerous reports showed applying DMSO to newborn rat skin protected them from damage from x-ray exposure, while in fruit flies, DMSO significantly reduced x-ray mortality and mutations of their sperm and in golden hamster embryos, DMSO protected them from gamma rays—the strongest form of radiation. DMSO has also been shown to prevent damage to mouse eyes following radiation exposure and to prevent the harmful (bystander) signals irradiated cells emit in their vicinity from damaging non-radiated cells (a fascinating phenomenon which I believe is mediated through mitogenic radiation). Likewise, DMSO has been repeatedly shown to reduce chromosome damage from radiation.
Note: DMSO has also been found to prevent damage from radiation therapy in non-cancerous cells and thus has been used as complementary cancer treatment.
•Neutralize harmful free radicals (e.g., those caused by radiation like hydroxyl) through scavenging charged ions (e.g., H+) and forming protective DMSO radicals. This, for example, was shown to be a mechanism behind DMSO’s ability to protect DNA from being damaged by radiation. Additionally, one study found DMSO prevented 80% of the DNA damage caused by gamma radiation and 100% of the DNA damage caused by a free radical generating system (which used iron and hydrogen peroxide).
Finally, due to these
protective qualities, DMSO’s toxicity is extremely low (e.g., due to the
immense scrutiny DMSO has been subject to, a large number of animal safety
studies were conducted, and in these, animals survived extraordinarily high
doses of DMSO). Many human studies have also been done, the
most significant of which involved 78 prisoners
over the course of 14 and then 90 days applying 1 g/kg to their skin (over 3-30
times the maximum amount of DMSO typically used) and then being subject to an
extensive battery of toxicology tests—all of which showed DMSO was safe. In
turn, despite millions of treatments having been given, no death has ever been
linked to DMSO (and the only two ever considered, one
in 1965, and one in 1994 did
not make a strong case DMSO was the cause of death).
Note: thousands of papers have been published on the biological effects of
DMSO and I have not yet found one that reported an adverse event from DMSO.
Because of that, I’ve mostly avoided mentioning each study I site here,
“detected no adverse events from DMSO.”
Along with the garlic
breath, the most common side effect (affecting 50-75% of users) is (reversible)
irritation at the site when 70% DMSO is applied topically on the skin (which
can be mitigated by applying a lower concentration of DMSO and frequently
decreases with increasing topical application), that occasionally after
prolonged used can lead to minor reversible changes in the skin (e.g.,
scaling). In roughly 15% of patients this skin reaction is marked and in 3.5%
it is significant enough that they stop treatment.
Less common side effects include nausea, increased urination, sleepiness, and
difficulty tolerating high IV doses. The most consequential (but fairly rare)
side effect is an allergic reaction to it (which affects roughly 1 in 2000
users—although it does not ever seem to manifest in an anaphylactic fashion).
Additionally, there is a high theoretical risk of a poison being on the skin
when DMSO is applied and brought into the body (hence why patients are advised
to wash their skin before applying DMSO) but significant instances of this have
been extraordinarily rare despite millions of DMSO treatments being performed
(rather the more common issue arises from using incompatible IV tubing which
DMSO can dissolve as it travels to the body). Lastly, it is generally advised
not to inhale DMSO (although it rarely vaporizes).
Circulatory Disorders
In addition to protecting
tissues from death, DMSO is remarkably effective at removing excess fluid from
outside the bloodstream, increasing circulation, and eliminating circulatory
obstructions (e.g., clots). As each of these issues comes up quite frequently,
DMSO is often extremely helpful in a variety of circulatory disorders.
For example, the
leading DMSO researcher found that 50% of patients
with Raynaud’s syndrome had their symptoms eliminated with DMSO and that
thrombophlebitis responds excellently to DMSO. Likewise, DMSO has been shown to
1. improve diabetic circulatory impairments such as peripheral neuropathy, or diabetic ulcers (where one study of hundreds of patients reported over a 94% treatment success rate) and
2. prevent future amputations.
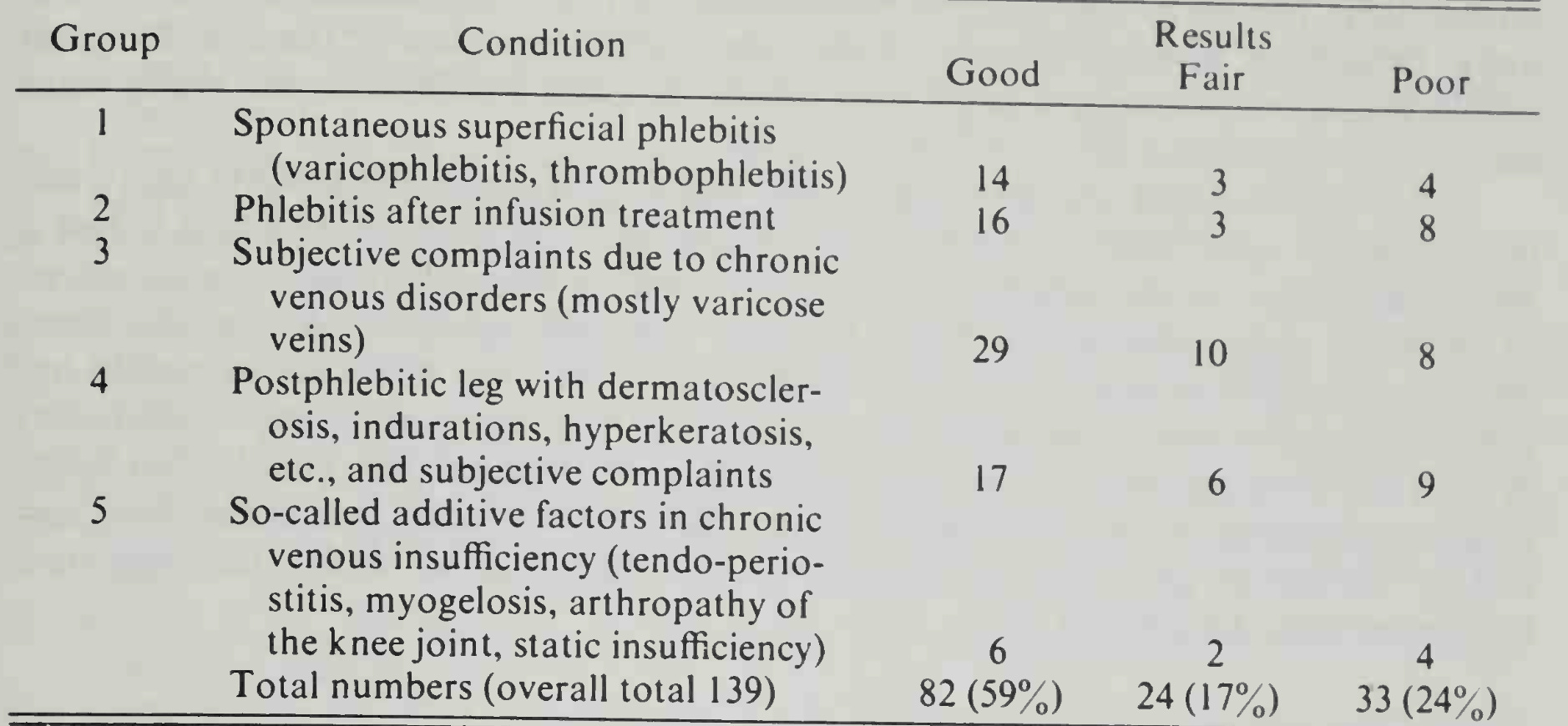
DMSO (topically and especially intravenously) is also quite helpful for varicose veins, in some cases improving the varicose veins within minutes and having the wiggly veins not reappear for months, which has been hypothesized to result from DMSO strengthening the vessel walls and their tone alongside generally improving venous and capillary circulation. Likewise, a study of 67 patients with varicose ulcers (39 females and 28 males), found they had a remarkable response to DMSO (even chronic ulcers which had been present for years).
Additionally, DMSO has been shown to help many other circulatory disorders:
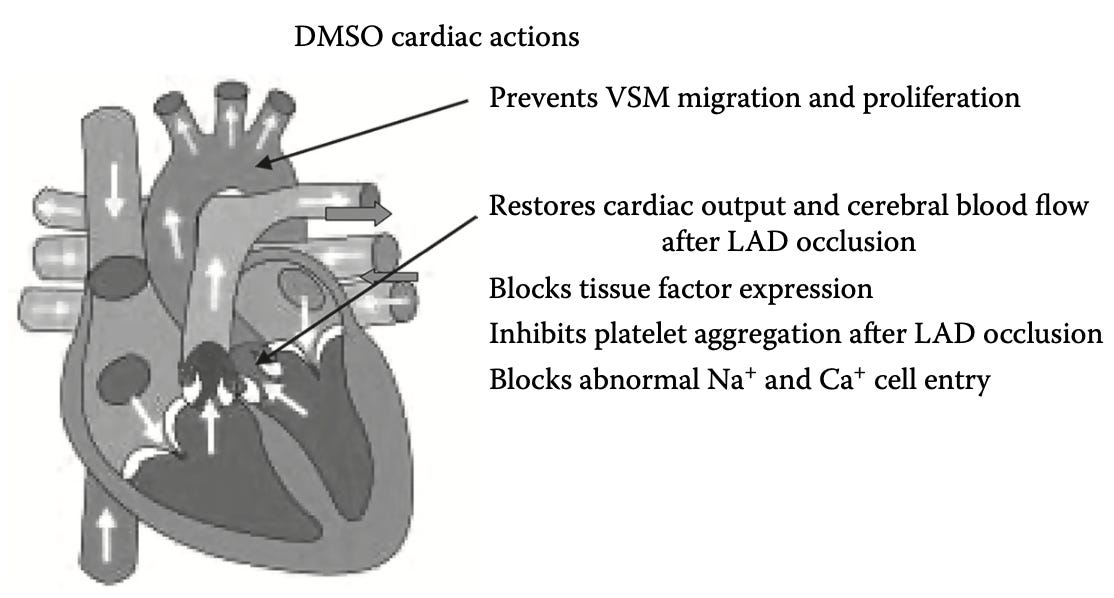
This is likely because, in addition to the previously mentioned properties:
DMSO can also increase or decrease the force of heart contractions (e.g., a 70 mM DMSO concentration or less has a positive inotropic effect, while a higher one can do the opposite or create a mild hyperpolarization that prolongs the action potential) in a manner independent of beta-adrenergic receptors, and does not alter cardiac rhythm. A slow infusion of DMSO can also cause a reduction of systemic vascular resistance and an increase in cardiac output (which was also shown in this study that simulated a heart attack).
DMSO prevents blood clot formation in the body and is a powerful platelet deaggregator (which prevents clotting). For example, it was found to reverse the reduction of coronary blood flow induced by a critical stenosis on the canine [dog] circumflex coronary artery without changing their other circulatory parameters, and it’s been shown with electron microscopy that DMSO prevented clots from forming at surgically blocked carotid arteries.
DMSO’s effects on platelets are thought to be
because:
•DMSO is a
sulf-hydryl inhibitor (which platelets need to bond) and a
hydroxyl radical scavenger (which also
inhibits platelet function).
•DMSO inhibits tissue
factor (TF) expression (a key part of clot formation—especially in the presence
of TNF-α), thrombus (clot) formation, and vascular smooth muscle cell
activation. TF (a platelet protein) is a key link between
inflammation and blood clotting.
•It increases cAMP (cAMP
inhibits platelet aggregators) by inhibiting one or more of the
platelet enzymes that breaks cAMP down (PDE2, PDE3,
and PDE5—which
is how many circulation improving drugs like Viagra also work, along with
certain cognitive improving ones).
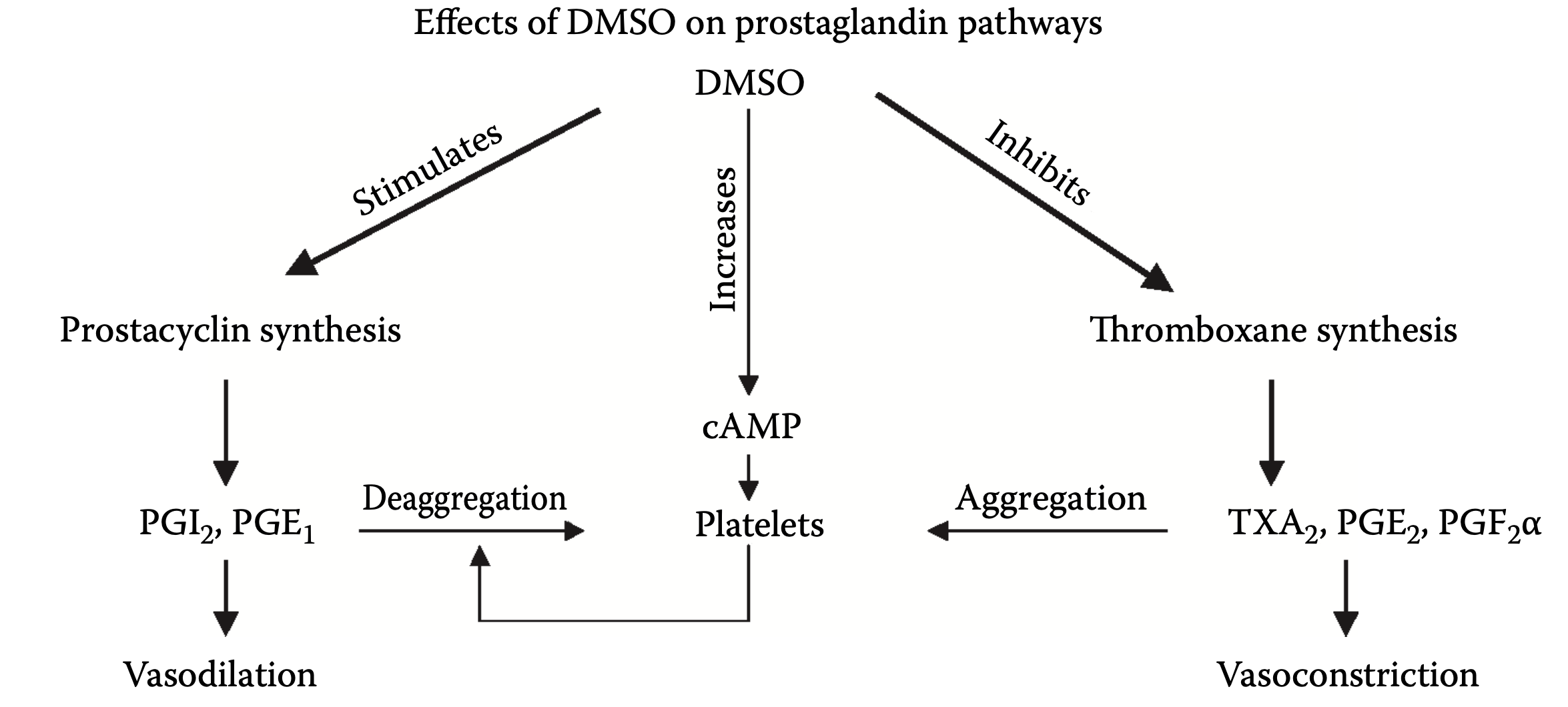
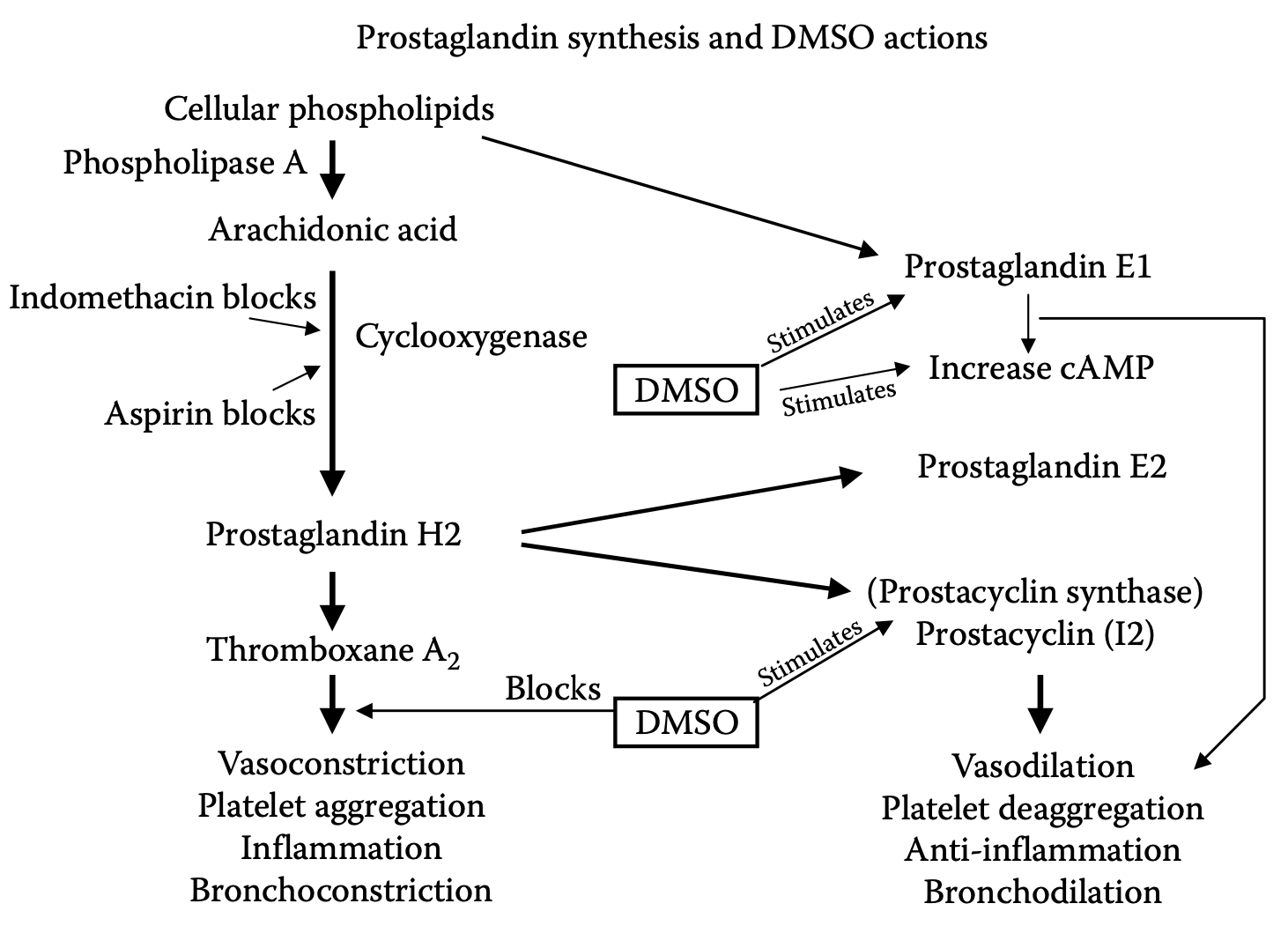
•It is a selective inhibitor of COX-1, it stimulates PGE1, and inhibits PGF2α, blocks PGE2 synthesis and likely blocks the release of thromboxane A2.
In short, DMSO provides a variety of anti-clotting activities which are similar to (but eclipse) the effects of aspirin and unlike aspirin, does not have any associated adverse effects, which leads to a remarkable number of potential uses for it (e.g., incorporating it into a drug eluting coronary stent). These charts in turn tie together much of the above:
Note: a review paper on this entire subject can be read here.
Heart Attacks
Given all of these protective and circulatory enhancing properties, DMSO appears to be an immensely promising treatment for heart attacks. Unfortunately, relatively little research exists in this area and likewise, a situation where it could be done does not frequently come up (e.g., by the time you start chest compressions it’s unlikely you’ll also be applying DMSO). Nonetheless, I have had colleagues who have cases of having successfully treated heart attacks with DMSO (or a zeta potential enhancing regimen).
In turn, most of the research that’s been done in this region has not happened in humans, but rather through stimulating a heart attack (e.g., by temporarily cutting off the blood supply in an animal’s coronary artery), and in those cases, the resulting damage to the heart was greatly reduced.
Note: the only other study I know that looked at this was an unpublished one (discussed here) where a total of 240 rats were given isoproterenol subcutaneously on two consecutive days which caused portions of the heart muscle to die and decay. Those who received 0.5 ml of 90% DMSO subcutaneously each day had much less heart damage and had no evidence of heart muscle aneurysm or rupture.
Additionally, a study attempted to model atherosclerosis by overloading rabbits with dietary cholesterol. It found that oral DMSO reduced the eventual atherosclerosis by 30-40% and halved the accumulation of cholesterol in the tissues.
Current Stroke Management
Roughly 3.1% of adult Americans have experienced a stroke (a figure I expect to rise from the COVID-19 vaccines). Each year, this translates to about 800,000 people in the United States having a stroke, and in 2022, 165,393 died (making it the fifth most frequent cause of death in the United States), with between 20-40% of survivors experiencing long term disability from the stroke.
Because of the harm strokes pose to society, and the rate at which brain tissue deteriorates once its blood supply is lost, the medical system emphasizes doing everything that can be done to identify and treat strokes as soon as possible.
Unfortunately, different types of strokes exist. In most
cases, the blood supply is cut off due to something (e.g., a clot) blocking the
artery (an ischemic stroke). However in 13% of cases it’s instead due to a
blood vessel rupturing and leaking out. This is problematic because the
primary treatment for strokes is to inject a powerful clot busting medication (tPA)
but in cases where the stroke is coming from a bleed, this can
be disastrous. As a result, nothing can be done until the patient is accurately
diagnosed (which requires a brain CT scan at the hospital), which in
turn results in an even longer delay before tPA can be used to save a patient’s
brain tissue.
Note: there are a few diagnostic signs that are more suggestive of a
hemorrhagic stroke (e.g., a severe headache or unusual neurologic symptoms),
but to our knowledge, no reliable method
besides a CT scan exists to differentiate the two.
Worse still, the statistics on tPA (approved in 1996 and still the only FDA approved treatment for ischemic strokes) aren’t actually that good. Presently, tPA is only approved to be given within 3 hours of a stroke starting (as its likelihood of benefitting a patient decreases with time)and in practice, it is often given up to 4.5 hours after symptoms start (since some degree of benefit still exists).
When that window is met (which only
happens about 25% of the time and ultimately results
in roughly 1.8%-8.5% of
ischemic stroke patients receiving tPA), the existing data shows that only
13% percent of patients who receive tPA significantly benefit from it
(39% return to normal, compared to 26% who would return to normal without
treatment), with an additional 19% of tPA users experiencing some degree of
improvement (but not a full recovery) from it.
Worse still, tPA can cause significant bleeding, which is sometimes minor
(e.g., gum bleeding), but also carries a 6.4% risk of
a symptomatic brain bleed, and a 1.6% risk of
a serious systemic hemorrhage (along with other issues such as a 1.3% to 5.1% risk
of angioedema and tPA frequently causing
reperfusion injuries). In turn, many risk factors exist for
the increased bleeding (e.g., a few common risk factors can lead to a 33% chance of
tPA causing a fatal bleed), and there have
been many lawsuits for either giving or not giving
tPA to a stroke patient. Additionally, tPA is a poor choice for larger
obstructions (e.g., one within
the internal carotid artery), which instead must be
physically removed. In short—many ICU doctors I know are quite hesitant to use
tPA as they have seen cases where it dramatically improved patients, many where
it did not do anything, and quite a few disasters (especially in the early days
of the therapy where it was used for heart attacks and then often caused the
patient to have a fatal or debilitating brain bleed).
Note: the best data exists for tPa being injected directly into the obstructed artery with interventional radiology. Unfortunately, while many premier institutions offer this, it is a specialized procedure that is not available at most hospitals.
Finally, there is essentially no therapy for recovery from stroke—which in short explains why stroke is the second leading cause of death and the third leading cause of disability worldwide.
In turn, it
would be paradigm shifting if an effective stroke therapy existed which:
•Effectively treated ischemic strokes.
•Had no risk of worsening a hemorrhagic stroke.
•Could easily be taken at home, and more importantly, be quickly given on
ambulances.
•Protected brain tissue from dying.
•Prevented reperfusion injuries.
•Healed damaged brain tissue after a stroke.
The fact that it’s been known DMSO does that for over 50 years (it’s even therapeutic for hemorrhagic strokes and can cross the blood-brain barrier to heal damaged neurons), in a nutshell, summarized why quite a few people I know harbor great animosity towards the FDA.
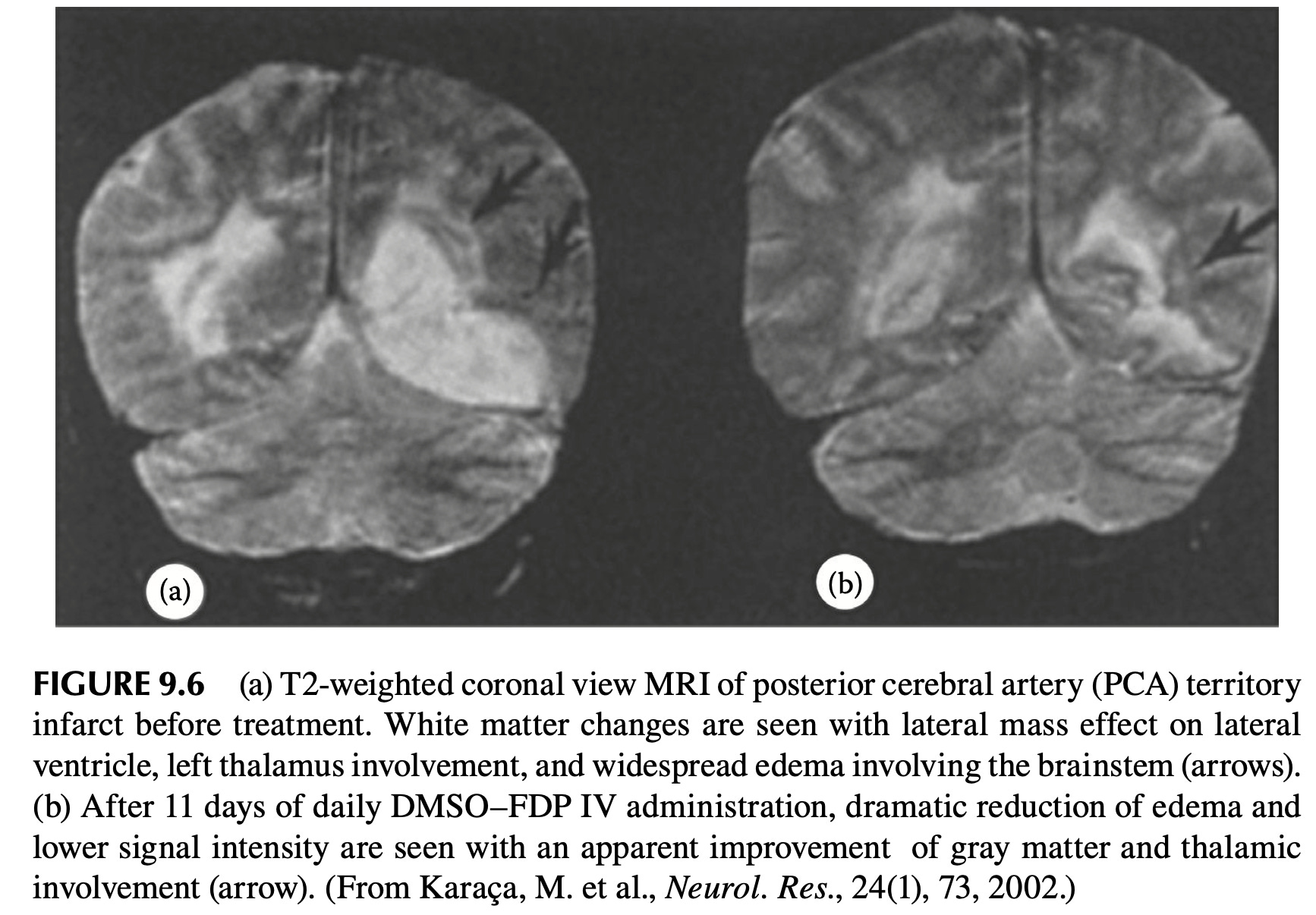
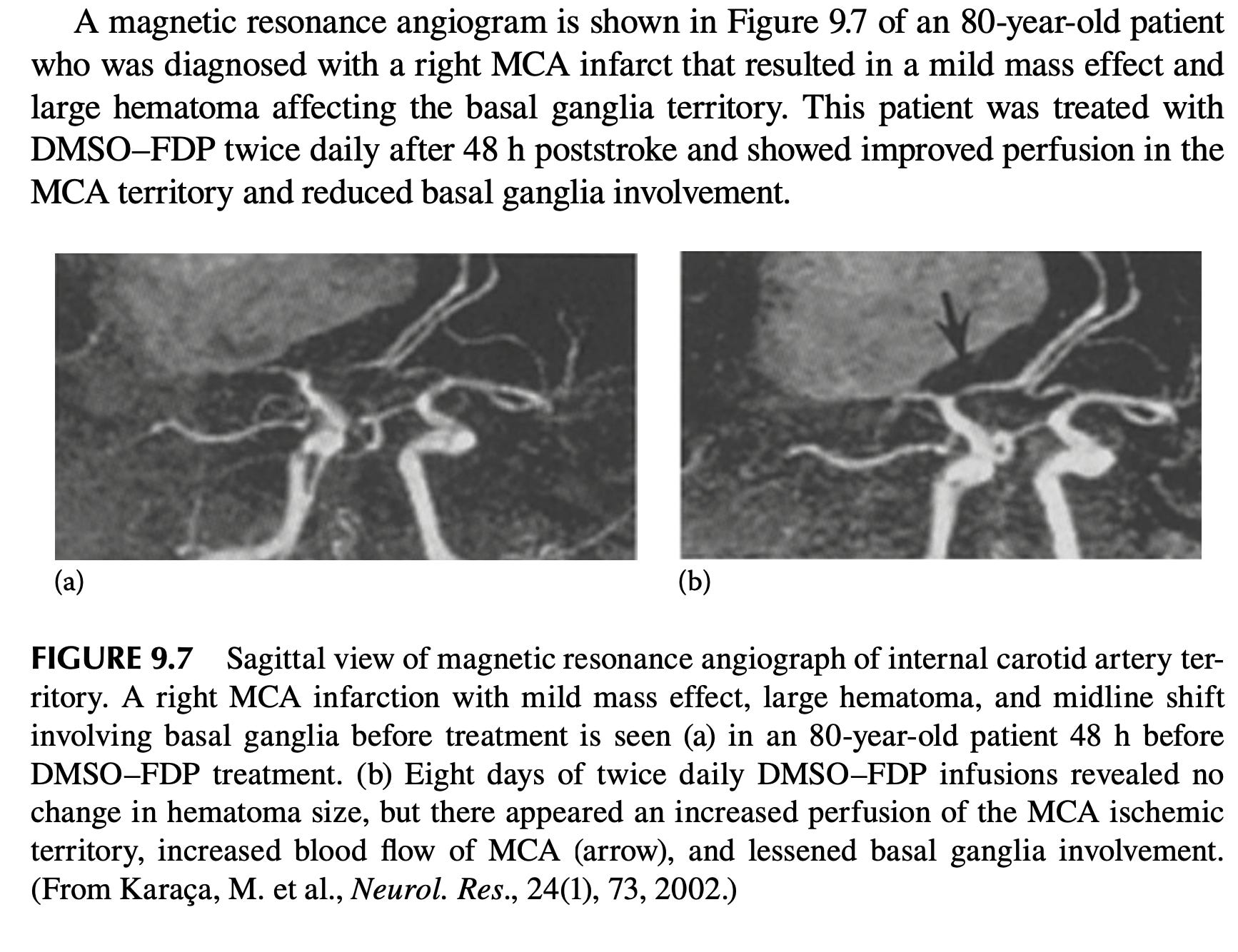
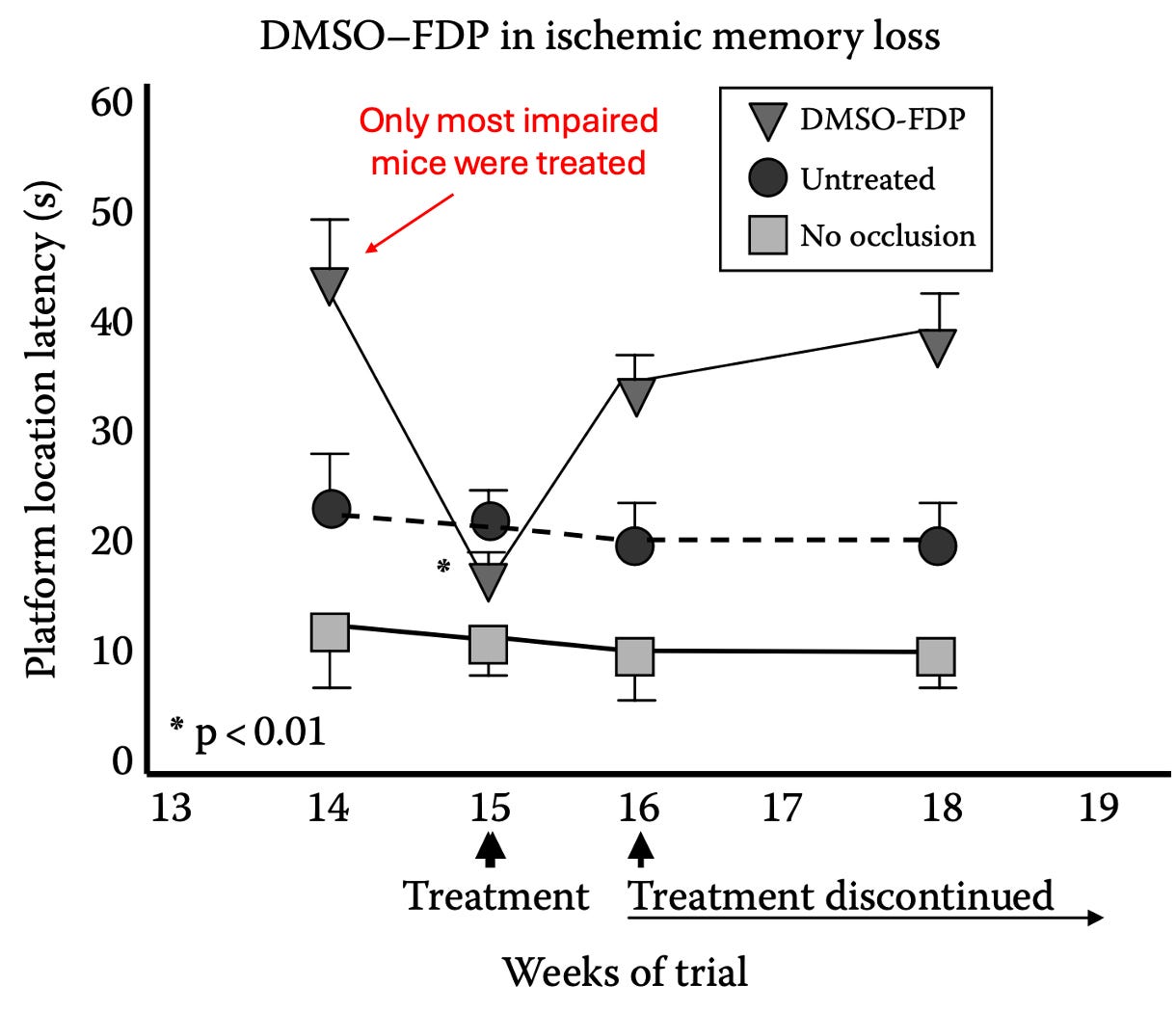
For example, a 2002 clinical trial (which can be viewed here) was conducted where DMSO and FDP (fructose diphosphate, a metabolite which cells turn into energy through glycolysis) mixed in 5% dextrose was administered intravenously twice a day (averaging 12 days) to 11 patients (average age 65) who presented with an acute or subacute ischemic stroke. After being subject to an extensive series of tests, it was concluded that DMSO was well-tolerated, that it benefited patients if given with 12 hours of symptom onset, and that 63% of the patients achieved 'improved' or 'markedly improved' neurological status (whereas for the patients receiving standard treatment, only 20% achieved an “improved” status three months later.
Note: since older patients are the most vulnerable to strokes and have had such a significant recovery (without adverse reactions), this indicates DMSO is an even more promising therapy for younger patients with strokes.
One of the most important aspects of this trial was that while DMSO is the most helpful when given immediately after a stroke, the trial showed DMSO could save the neurons long after the stroke had happened.
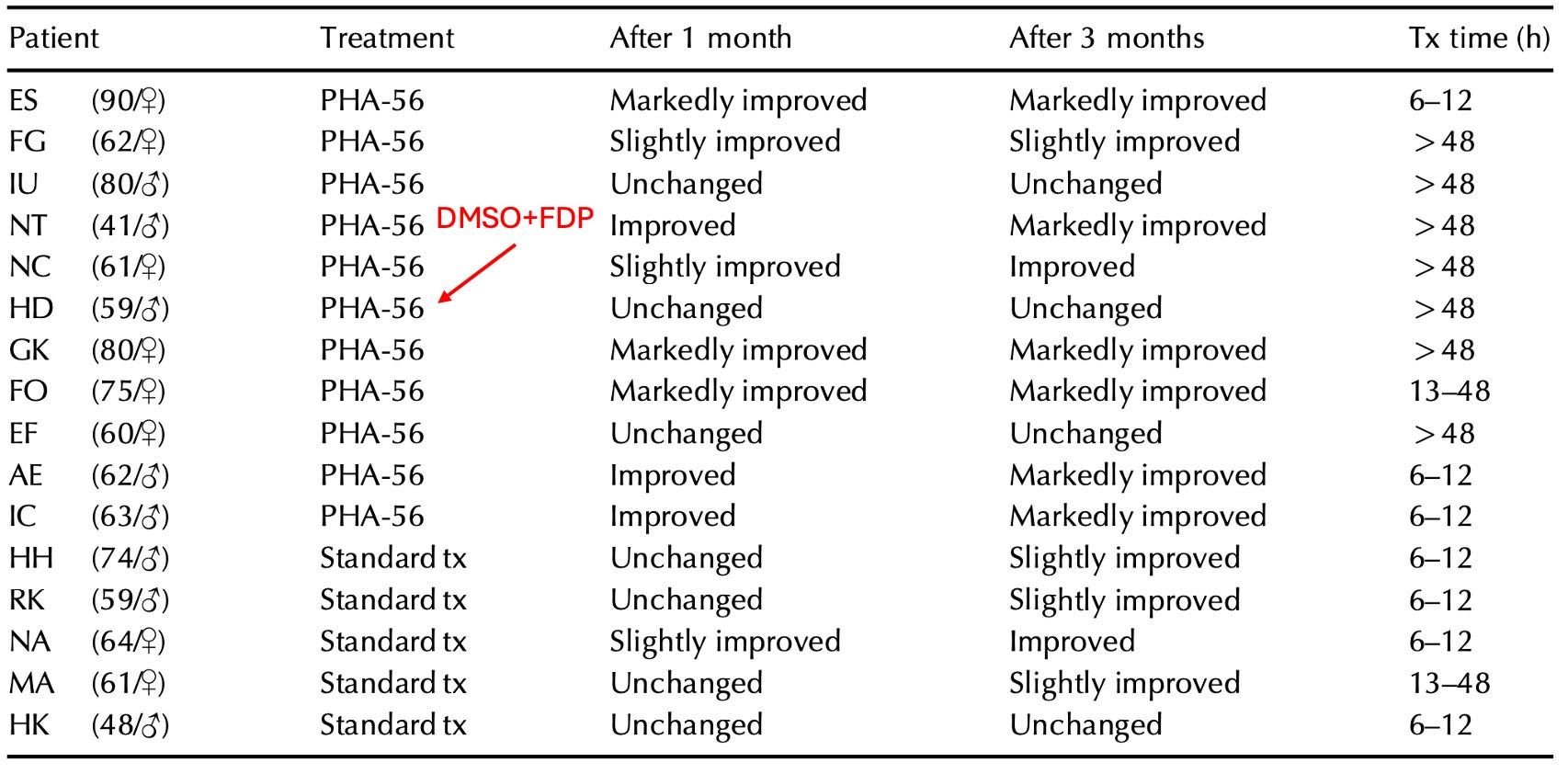
“Tx time” designates how long after the stroke symptoms treatment was initiated.
Given the existing options for strokes, a trial like this should have been immediately replicated by premier institutions around the world—but instead almost no one even knows it happened.
Note: there are also animal studies on the DMSO-FDP mixture.
- In a rabbit study, blood flow to their brains was cut off (via hypoxemia, hypotension, and a bilateral common carotid artery occlusion), which eventually caused them to develop isoelectric (flatlined) brainwaves. After 5 minutes of no brain activity, they received either DMSO and FDP or saline, and then after roughly 2 minutes had their blood supply restored (with the DMSO group having an extra 1.4 minutes of no blood flow). The DMSO group regained brain activity much faster (a result frequently seen in animal experiments), all survived and all had minimal brain tissue damage, whereas only 22% of the saline group survived (and were severely disabled with significant brain tissue damage).
- In a mouse study (which can be read here), mice were subjected to moderate or severe head impacts and then treated 5 minutes later with various compounds, then evaluated for motor function (via a grip test), brain tissue damage, and survival. DMSO-FDP was the most protective, DMSO the second best, while the rest (e.g., FDP alone) did not provide a benefit.
Ischemic Strokes
After I learned how unconscionable the FDA’s prohibition against DMSO was, I made a point to begin telling people (e.g., friends, relatives, patients) I felt were at risk of a stroke to stock DMSO at home, and since then, I’ve had instances where someone (or their caretaker) called me up, described a stroke, I gave them instructions on what to do (since they already had DMSO at home), and by the time they got to the ER, the stroke was “resolved” and in some cases, the ER was confused by the CT scan because it both looked like a stroke had happened and simultaneously that one had not.
Note: in my opinion, IV DMSO would have been ideal (and more effective) in those situations, but in each case, it was not feasible to implement.
Likewise, many compelling cases have been recorded of individuals who treated their strokes with DMSO:
A Los Angeles school teacher had a major stroke shortly after the start of the Christmas break. She was unconscious on her living room floor. DMSO treatment was started immediately after the stroke. The DMSO was first applied topically to her head within minutes of the stroke. Less than one hour after the stroke she was given DMSO by intramuscular injection. This patient was never taken to the hospital for this stroke. A prominent surgeon who was a family friend told the husband of this patient that it was important to keep her out of the hospital. The surgeon said that even though the treatment was completely legal, it would be difficult to get approval to give the DMSO especially by injection at his hospital.
This patient made a dramatic recovery. She regained consciousness later in the day in which she had her stroke. Treatment continued for the next week. Each day she received two topical applications of DMSO, one intramuscular injection of DMSO, and two doses of one teaspoonful of DMSO in juice. Her condition improved each day. When school resumed after the first of January, this teacher was back in the school teaching the students as if nothing had happened during the Christmas vacation. She never even mentioned it to the other people at the school. She continued teaching until she retired. She retired healthy with no disability.
Note: if you drive someone to the ER (and call in ahead to let the ER know you are coming), you have numerous opportunities to administer DMSO prior to placing the patient in the ER without delaying their care there (e.g., emergency brain surgery for a hemorrhagic stroke).
A lady was in a coma in a convalescent hospital and had been in the coma since her stroke three months ago. She was given little chance of recovery and was expected to remain in a vegetative state until her death.
When I first observed this lady, there was no response to any type of stimulus. She was alive, but appeared lifeless. It was decided that her treatment should be topical DMSO applied to her head daily either by her husband or by one of the nurses at the facility.
One month after the start of treatment, there were positive signs in the lady. Her brain was starting to respond to the DMSO. The treatment continued, and four months after treatment started this lady was able to return to her home. After her return to her home, this patient started drinking one teaspoonful of DMSO in a small glass of water each day in addition to the daily topical treatment. This treatment continued for a period of years.
Three years after the start of DMSO treatment this writer returned to visit this patient. At this time the lady was living a normal life, not the life of a stroke victim. She was able to look after the house and walked normally.
The only lingering effect of the stroke was a slight speech defect. At this time she said that her memory was better than that of her husband who had not had a stroke and who was considered to be completely normal.
Note: there are also many reported cases of individuals who took DMSO for musculoskeletal or pain disorders (by far the most common use of DMSO) who then experienced a permanent improvement of stroke symptoms.
As shown earlier in this article, DMSO has numerous properties that make it uniquely suited to protect from the damage of ischemic strokes. These benefits have in turn been shown to occur for brain tissue. For example:
DMSO was shown to preserve the neurological function of brain tissue samples once their oxygen or glucose were withdrawn (with similar results seen in this study).
Giving DMSO to
rats 30 minutes prior to cutting off the blood flow in their MCA (a key artery
in the brain) significantly reduced the amount of permanently damaged brain
tissue. Additionally, this study and this study had
similar results.
A more recent
rat study found giving DMSO 20 hours before blocking the MCA reduced
the damaged brain tissue by 65%, by 44% when given an hour after, and by 17%
when given two hours afterwards.
Note: these results argue
that giving IV DMSO beforehand could reduce the complications of many
challenging surgeries (e.g., a coronary bypass). Unfortunately, much in the
same way ultraviolet
blood irradiation dramatically reduces bad surgical outcomes,
neither has been adopted for this purpose.
A gerbil study (this species
is more susceptible to strokes) found blocking carotid
blood flow to the brain and then restoring blood flow to the brain caused
significantly less neuronal loss if DMSO was given 30 minutes before the
carotid blood supply was cut off. Another gerbil study had
similar results.
A dog study cut off cerebral blood flow, then restored it and used a variety of biochemical measurements to monitor cellular metabolism (along with EEGs). Dogs who received DMSO (and an anti-platelet agent) had significantly higher mitochondrial function (which was almost identical to controls who had not suffered the occlusion).
Another dog study induced a stroke by introducing an embolus (clot) into the MCA and then giving DMSO. Compared to controls, those given DMSO were observed to have normal behavior and no neurological deficits afterward, whereas 3 of the 9 controls died (with significant tissue death in the brain), while the survivors had contralateral paralysis (a typical stroke consequence) and impaired consciousness.
A cat study found DMSO protected brain tissue from MCA occlusion and increased cerebral blood flow (CBF) by 27%. When DMSO was given in conjunction with PGI2, a greater improvement was seen (e.g., a 68% increase in CBF).
A rhesus monkey study blocked the MCA for 4 hours, gave DMSO, dexamethasone, or nothing, and then opened the MCA after it had been blocked for 17 hours. DMSO gave significant protection from the severe neurological deficits and loss of arterial blood flow the other two groups developed.
A squirrel monkey study blocked the left MCA for 4 hours, and then given a variety of different treatments (e.g., saline, hemodilution, or hyperbaric oxygen at 2 atmospheres). Seven days after treatment, 8 of 10 DMSO treated monkeys were alive (with 2 having mild contralateral muscle weakness), while 75% of those receiving hyperbaric survived, and 34% of those receiving hemodilution (with the last two groups also having more significant neurological deficits). Finally, combining either of these treatments with DMSO produced slightly worse results than just DMSO alone.
Lastly, a rat study found that when hemorrhagic shock was induced, DMSO downregulated the inflammatory response (NF-kappaB) and unregulated a key protein cells use for survival (HSP70).
Note: small strokes can still cause significant long-term issues (which DMSO often completely prevents), so as a general rule, I advise using DMSO anytime someone has a suspected stroke.
Hemorrhagic Strokes and Traumatic Brain Injuries
While ischemic strokes are difficult to treat, hemorrhagic ones (and other traumatic brain injuries) are even more challenging, and after decades, there has been surprisingly little progress in neurologic intensive care, particularly in preventing long-term paralysis and disability.
Note: conflicting evidence exists supporting the use of progesterone, hypothermia, and hyperbaric oxygen therapy for traumatic brain injuries, but none of these approaches are in widespread use. Strong evidence also supports the use of methylene blue but it also is rarely used. Finally, certain trials (e.g., with progesterone or with an adenosine kinase inhibitor) find those therapies work even better if combined with DMSO.
It was, as if the hand of God had somehow touched the [experimental] animal’s forehead. ‘I don’t believe it’, I stammered. But it was true. I felt a tingling in my spine because this reawakening of a virtually dead animal had all the markings of a medical breakthrough [Jack de la Torre MD].
Instead, the discovery, the potential for saving lives and the continued research that should have uncovered other uses for dimethyl sulfoxide and similar agents was quietly laid to rest in the coffers of forgotten medicine.
Note: Torre’s observations were partly based on the fact he saw numerous animals with flatlined EEGs (which typically precede brain death and then actual death) have the EEGs come back within 10 minutes of receiving DMSO.
When treating severe brain bleeds, a few major challenges exist.
First,
swelling and the leaking of blood into the brain can dramatically increase the pressure on
the brain (known as intracranial pressure or ICP). The brain’s tissue in turn
is very sensitive to increased ICP or masses (e.g., a large blood clot)
compressing it. Unfortunately, there is no good agent for reducing ICP
(e.g., the most commonly used agents like mannitol can create a “rebound ICP”
which is higher than it was at the start).
Note: there can also often be a breakdown of the blood brain barrier which
causes even more fluid to enter the brain.
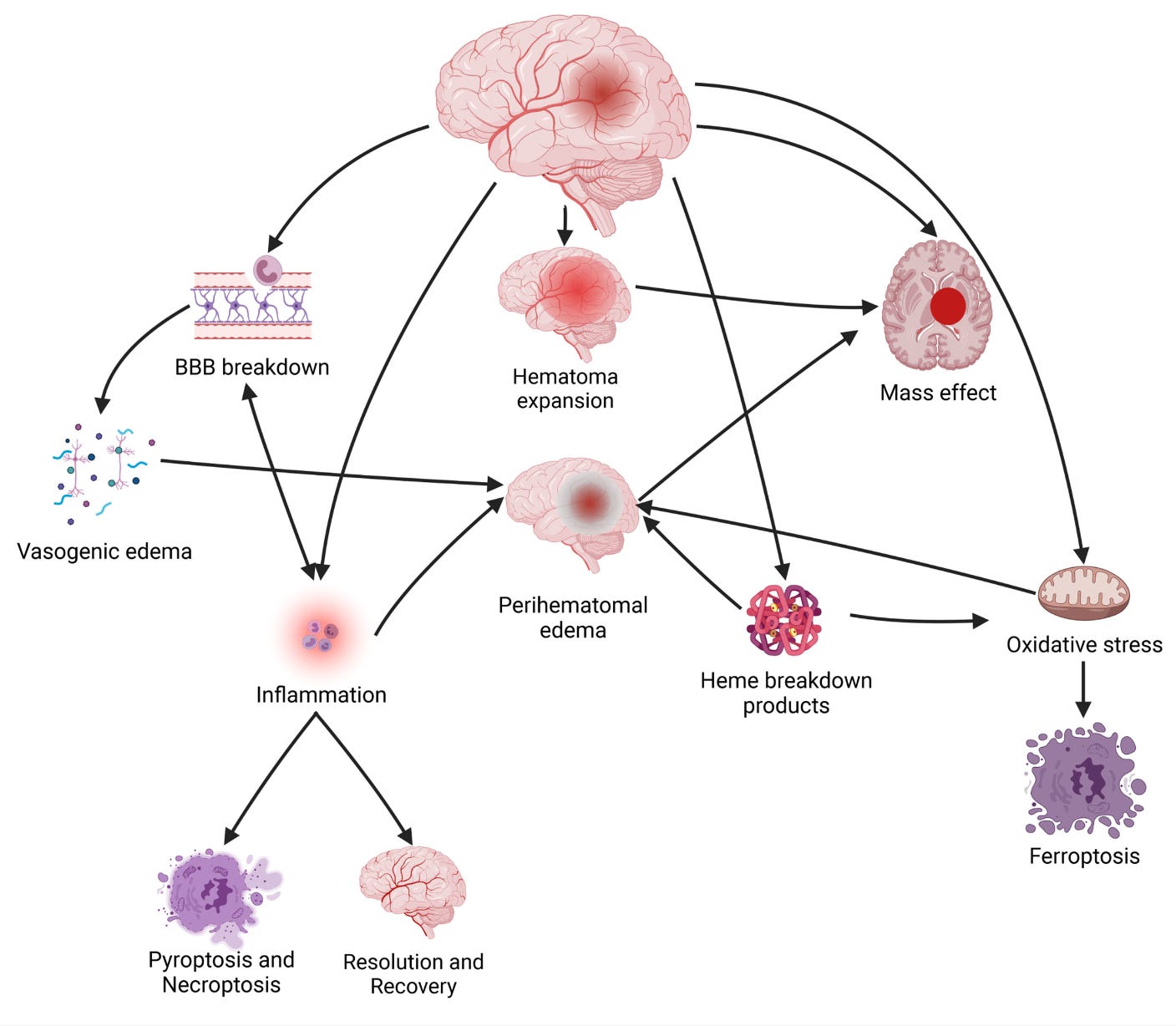
Additionally, inflammatory processes begin once the blood enters the brain which injures brain tissue (and triggers cell death), while simultaneously, the iron released by dying blood cells generates free radicals which then destroy brain cells.
Remarkably DMSO addresses
each of these issues. For example, it rapidly lowers ICP (without
the risk of a rebound) and unlike many other ICP lowering agents, does not cut
the blood supply to the brain (rather it increases cerebral perfusion without increasing blood
pressure or heart rate—which is important because brain cells
rapidly die without a sufficient blood supply to maintain their metabolism).
Likewise, improved cerebral blood flow is necessary to remove the blood that
leaked into the brain (with DMSO in turn being excellent for reducing
brain edema). Finally, DMSO lowers many of the
inflammatory cytokines (e.g., IL-1α, IL-1β, and
IL-6) associated with
strokes and tissue injury (along with macrophage
chemoattractant protein-1).
Note: I suspect rebound ICP is the brain’s attempt to get enough blood, and
since DMSO ensures this, that’s why it doesn’t cause rebound ICP.
In short, as far as I know, no comparable agent exists for lowering ICP (one of the greatest challenges in neurocritical care), and in turn, many (unsuccessful) agents have been tried (in part because what works in animals often does translate to human brains).
Note: one monkey study that compared mannitol to DMSO in experimentally induced missile (bullet) injuries found DMSO created significantly better cerebral perfusion, and had a 86% survival rate (vs. 75% for mannitol and 55% for the untreated group).
Furthermore, beyond directly removing edema (water) from the brain and bringing it back to the bloodstream (which is how it lowers ICP), limited experiments done in humans show DMSO is somehow able to reduce the spilling of blood into the brain (the mechanisms of which has not been worked out).
Additionally, DMSO also addresses many other critical aspects of traumatic brain injuries and brain bleeds (which under conventional care requires many different drugs):
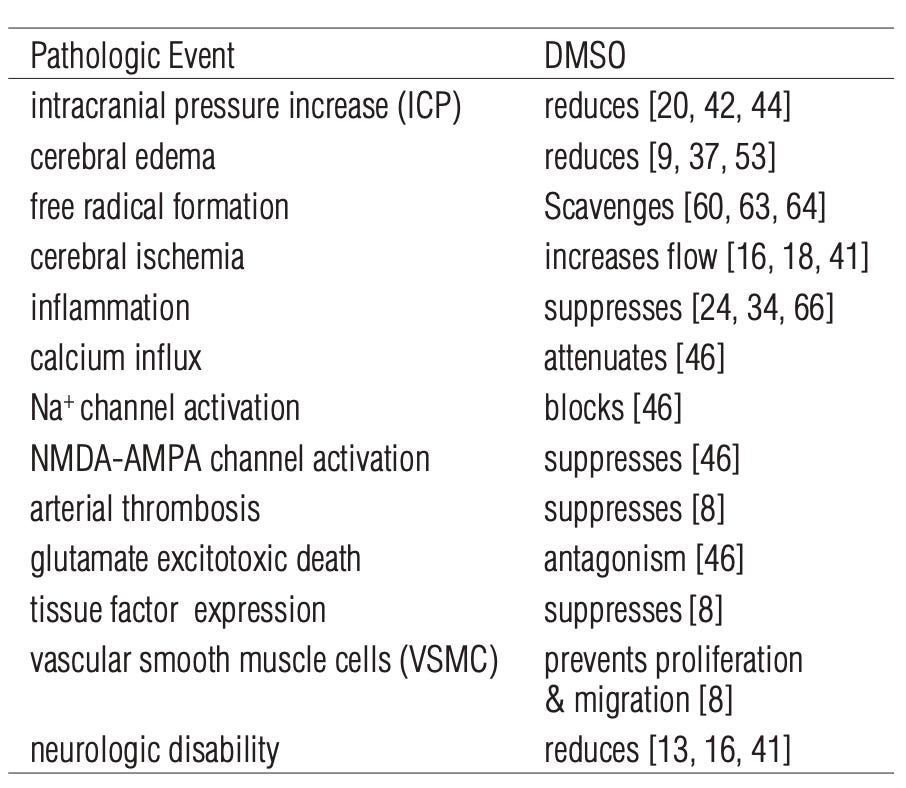
The sources for each of the above citations can be found here.
Note: DMSO also lowers the JAK2/Stat pathway, suppresses neurotoxic NMDA-AMPA-induced ion currents, prevents iron induced lipid peroxidation and focal edema, and as mentioned above, protects cell membranes.
A variety of studies have been conducted that demonstrate DMSO’s remarkable therapeutic potential in these situations:
•Ten patients with closed head trauma and elevated ICP (40-127 mmHg compared to the normal 5-13 mm Hg) received IV DMSO, with an ICP drop in most cases happening within 30 minutes, and averaging 28mmHg after 24 hours, and 58mmHg after six days. Most patients then took 2-10 days to have the fluctuations in their ICP diminish (this study can be read here).
The reduction in brain swelling following DMSO treatment was confirmed by CT scans. All patients had a neurological assessment six days after the DMSO treatment. Six patients had mild or no problems, two had moderate impairment, and two had severe impairment (two patients eventually died of their injuries). Three months later, seven patients had minimal to no impairment, while one patient showed no improvement. No adverse effects from DMSO were observed.
•A follow-up study (at the same hospital) of 10 patients with severe closed head injuries (causing brain edema and increased ICP) found DMSO rapidly reduced ICP, increased cerebral perfusion without affecting the systemic blood pressure and patient responsiveness (except only in one patient), and most importantly improved the neurological course and outcome of the illness.
•A study examined
11 adult patients with high ICP and a GCS score of 4–6 following brain trauma
or subarachnoid hemorrhage (standard therapy did not work) who were on the
verge of dying. DMSO was then given, which immediately reduced the ICP (and
induced diuresis), with 3 (who had been expected to die) then surviving.
Note: it was also concluded this study demonstrated the value in keeping the
cerebral perfusion pressure above 60mmHg (something DMSO helps with) even in
the presence of high ICP.
•One paper reported on nine patients who suffered a partial or total hemiplegia (paralysis) after surgical repair of an aneurysm:
- In a 61 year old male (R. MCA and R. carotid), DMSO was initiated after surgery due to blood pressure climbing and left-sided paralysis developing, and in 30 minutes, blood flow increased in the right brain region by 20% (and 11% on the left), the patient’s condition greatly improved. DMSO was then stopped day 5, and paralysis (and confusion) rapidly came back, after which DMSO was resumed and the patient fully recovered.
- A 67-year-old woman (L. MCA) lost the ability to speak and developed right-sided paralysis after surgery. After 8 hours DMSO was started (as mannitol didn’t work), and within 45 minutes she became fully alert and regained her strength, within 2 hours her cerebral blood flow improved, and within 12 hours her motor strength permanently normalized.
- A 25-year-old woman was hospitalized with severe headache and high blood pressure from a L. MCA aneurysm (and spasm in the internal carotid). 12 days after surgery, she suddenly developed right-sided weakness, right-leg paralysis, and difficulty speaking. After 8 hours of mannitol didn’t help, DMSO was started, and within 90 minutes she could lift her leg, and by the following day she had fully recovered.
- A 28-year-old woman developed excruciating headache and right sided weakness from an MCA aneurysm who then developed a severe internal carotid spasm that did not respond to standard care but did from DMSO (allowing her to have a completely recovery).
- The remaining five cases of a hemorrhaging aneurysm had a similar course to the above cases after rapidly responding to DMSO, with all but one patient (who had a variety of severe exacerbating factors) making a full recovery. Additionally, no adverse events were observed in any cases.
•Finally a report discussed by Dr. de la Torre (which I could not locate), detailed five patients with closed head injuries and a high ICP which rapidly lowered from IV DMSO. A 1.5 year old with a GCS of 7 and ICP of 30mmHg fully recovered over 3 weeks, while a 7-year old child admitted with a GCS of 5 and an ICP of 25 mmHg fully recovered after 8 weeks at the hospital. The three other patients (aged 17-52 with GCS scores of 3-5 and two having ICPs above 50 mmHg) initially responded to DMSO but did not survive.
Note: in animal experiments simulating severe brain injury, DMSO has also been shown to strengthen their respiration (whereas in many cases it instead becomes shallow and may eventually stop). Additionally, in both humans and animals, DMSO (due to it functioning as a diuretic) will often significantly increase urination.
Animal research in turn supports the above results:
•A rabbit study created lethal brain edema (and increased ICP) by freezing part of the brain. DMSO was observed to significantly reduce ICP after 5 minutes while increasing cerebral perfusion and not changing central venous pressure. This was then followed up with a study that achieved similar results with a different DMSO dose and a final study that showed indomethacin blocked DMSO’s reduction of ICP.
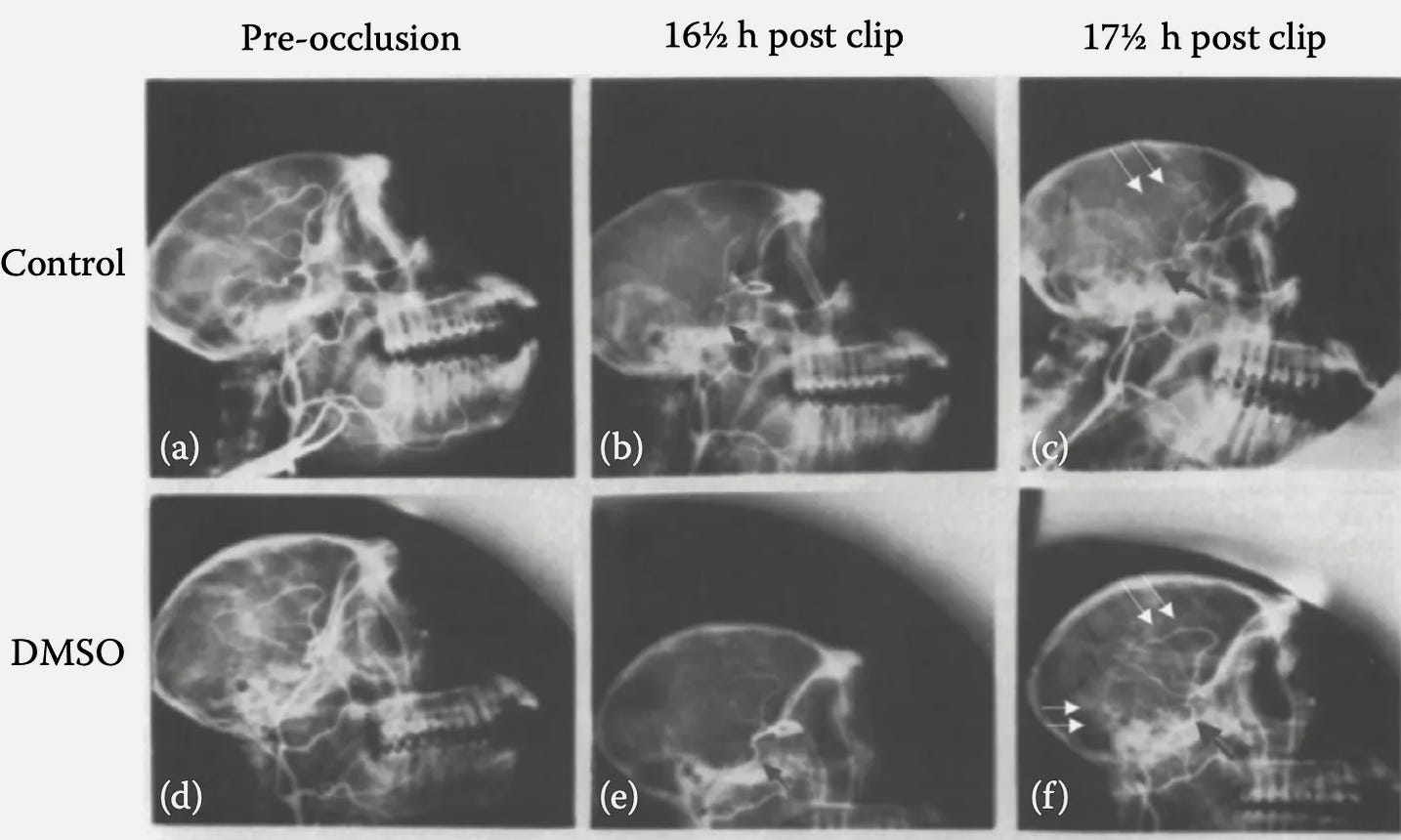
•A monkey study, had an expanding balloon (designed to stimulate a hematoma) was placed in the brains of 40 monkeys, 15 of whom received DMSO. Of the DMSO treated monkeys, 1 (7%) died, and 1 developed mild right side paralysis. In contrast, 90% of those who received saline died (with the survivor having severe neurological deficits and dying the next day).
Note: in animal experiments simulating severe brain injury, DMSO has also been show to strengthen their respiration (whereas in many cases it instead becomes shallow and may eventually stop). Additionally, in both humans and animals, DMSO (due it functioning as a diuretic) will often significantly increase urination.
To put all of this into context:
A January 11, 1981, a news report in the Ocala Star Banner [page 6], carried the headline: “DOCTOR CLAIMS DMSO SAVED 11.” The story read:
SAN DIEGO (AP)—A doctor at the University of San Diego credits the controversial drug DMSO with saving the lives of 11 people who suffered severe head injuries.
Dr. Perry E. Camp, a UCSD Medical School neurosurgeon, said Friday that dimethyl sulfoxide was effective for 11 of 30 people judged near death and for which other lifesaving methods have proved useless.
“To take patients like that and have even one out of 10 survive is phenomenal,” Camp said. “The fact that we have any survivorship at all . . . doesn’t sound like much, but it is extremely encouraging,” Camp said.
Sadly, however, despite the immense amount of research conducted and these results being dramatically better than what the standard of care can offer, this remains an almost completely forgotten side of medicine. That said, one treatment for brain bleeds (Onyx) is composed of a polymer dissolved in DMSO which solidifies into a solid coating which “patches” the leaking vessel.
Click below to share this post!
Concussions
Many of the same principles hold true for concussions, and the pioneers of DMSO felt it was an essential treatment for athletes after they experienced one—particularly since concussions can predispose the athlete to long-term cognitive issues (e.g., both boxers and professional football players have a threefold risk of dementia).
One study for example applied pressure to the brain that was sufficient to cut off its blood supply (in an attempt to mimic a concussion), with DMSO being administered prior to this and every 12 hours for the next 3 days. DMSO was compared to other commonly used agents and found to be the most effective at preventing nervous tissue damage and neurobehavioral changes. Additionally, this study demonstrated giving alcohol beforehand (a common factor in drunk driving) increased the damage that the “concussion” caused (which DMSO alleviated).
In humans, there are also periodic cases of dramatic concussion recoveries following DMSO. For example, one author shared the case of a woman who had received a severe concussion from falling off a horse, after which she had trouble walking, would suddenly neurological decompensate (e.g., she would drop something), and had memory issues alongside foggy headaches. Thirteen years later, she received an injection of DMSO, immediately had a large improvement, and further improved with subsequent injections.
Spinal Cord Injuries
We used to think that the damage caused at the moment of injury in a severe head or spinal cord injury was irreversible. But now there are animal studies and a handful of clinical cases that tell us something different. There is still a little bit of time before the injured cells die. Based on what we’ve seen in animal studies and a handful of human situations, we think that if you can treat a head injury victim within a few hours of the injury, or a spinal cord victim within one hour, there is a good chance of preventing death or the paralysis that would otherwise occur.—Dr. Jack de la Torre“
Since central nervous tissue
does not regenerate, classically, strokes and spinal cord injuries are
considered to be incurable (e.g., despite decades of research, the standard of
care is still using steroids—despite the
existing evidence showing they don’t work and them having
many side effects).
Note: one survey
found that the primary reasons spinal surgeons use steroids for
spinal cord trauma is to avoid being sued.
As much of the same pathology that causes permanent damage in the brain also occurs in the spinal cord (the loss of blood flow and compressive post-traumatic swelling), DMSO can produce miraculous results. In turn, when the pioneer of medical DMSO, Stanley Jacob MD, was asked who would benefit the most from DMSO being adopted by medicine, his response was immediate:
'As I get to know the quadriplegics, ever so many of them eventually will say to me, 'You know, Dr. Jacob, I couldn't even commit suicide.'
In turn, like strokes, the greatest benefit from DMSO is seen if it is given (intravenously) within 90 minutes of the injury (e.g., de la Torre found that giving DMSO to dogs shortly after a spinal cord injury that typically produced permanent paralysis were spared from it and regained almost normal function within a few weeks). Likewise, the sooner to an injury, the more dramatic the improvement is:
At this time, Jacob was treating eight quadriplegics; and of them only one had presented a recently incurred injury. He felt, as do most doctors, that treatment is more fruitful in new than old conditions. The one fresh case was that of a sixteen-year-old girl, a fine athlete, who dove off a board and landed on her neck on the bottom of the pool.
Her doctor was pessimistic but willing to try almost anything that offered a glimmer of hope. She was a complete quadriplegic—utterly helpless.
She was on DMSO for an entire year. Gradually—one by one, it seemed—her organs began to function again. Eventually she walked. And now she is in college, doing very well.
However, at the same time, DMSO can often provide significant rehabilitation for far older injuries.
An Orange County, California, engineer suffered a severe back injury in an automobile accident. He was paralyzed below the point of injury and was confined to a wheelchair. However, his spinal cord was not severed. It did suffer damage, but there was no break. DMSO treatment was offered, but this man refused the treatment. He was convinced that it would not work, and he would never walk because a few months after the accident he still had no feeling in his legs.
Twelve years after the accident this man changed his mind and decided to try topical treatment with a DMSO lotion. The lotion was applied twice a day to the entire back of this patient. After three months this man was able to move the toes on his right foot. He never regained the ability to walk, but the treatment restored some feeling and the ability to move a part of his body below the injury site.
Our son had been in a coma due to an auto accident. After six months in the hospital we brought him home. His Drs. said that he would probably never regain bladder control. In 1973 he became a patient of Dr. Jacob. Within months of using DMSO he had full bladder control.
“We have had experience at our medical school in Oregon with two patients in which DMSO was given as early as an hour after what was considered an irreversible injury—an immediate, complete quadriplegia—and in both people there was total recovery with them walking out of the hospital,” said Dr. Jacob.
The neurosurgeon told me [his mother] that henceforth Grey's only motion would be to move his head from side to side and grin [due to a C4-C5 fracture that had blocked the cord there]…Grey listened attentively and thought a minute; then said to the doctor, "One day I will swing my legs off my bed and I will offer to bet you I am going to walk. At that time, put your money where your mouth is now.
In insisting that her son
would find help, Dorothy Keinsley did not delight all the doctors. "One
doctor bellowed at me like a bull moose in rutting season," she said.
"Don't you know your son is paralyzed?" He screamed. I explained that
no one knew it as well as I."
Grey read Ann Sullivan's article about DMSO…He wrote to Jacob, and his
physician made the tests Jacob had required. On February 13, 1965, Jacob came
to [Gray’s] Littleton [CO] home free of charge and swabbed Grey's neck with DMSO.
'The most dramatic change happened that first day," Dorothy told me.
"Grey had had a constant pain in his right shoulder from the time of the
accident, and he had learned to live with it. Late that day, Grey discovered
the pain had gone. He was almost incredulous. He expected the pain to return,
but it never has.
"Other improvements were gradual, as Dr. Jacob had predicted they would be.”
Note: Gray made remarkable improvements which eventually stopped (but did not regress) due to the FDA unconscionably revoking the medical use of DMSO.
As far as I know, while many
compelling cases (e.g., those just mentioned) exist, unlike strokes and severe
blunt head traumas, no formal studies on DMSO after spinal injuries have been
conducted in humans. However, as shown previously, mechanistically there is evidence
to support that use, and a variety of corroborating animal studies, all of
which led
the leading researcher in this field to conclude that
if a severe spinal cord trauma is treated with intravenous DMSO within 2
hours, paralysis may be
prevented.
Note: animal studies also showed the greatest benefit from DMSO
occurred if it was given
within 2 minutes, and that higher DMSO doses also
increased the speed and likelihood of recovery.

Scale: 0 = flaccid paraplegia, 1 = some muscle tone, 2 = reflex standing, 3 = spastic walking, 4 = walking, running with deficit, 5 = normal, full recovery
Note: I was unable to view the referenced study, but I was able to find an earlier version of the above data here.
Numerous other studies (e.g., in cats) have demonstrated that DMSO is superior to any of the other available options for spinal cord injuries. For example:
•One investigator found that
after transecting rat spinal cords a variety of changes occurred
in the spine which were mitigated by DMSO (e.g., it was hypothesized
that DMSO removing fluid pockets commonly seen after spinal cord injuries
created space for nerves to regrow).
•In one study
where T5 was transected, DMSO following the injury was found to
be superior to both hyperbaric oxygen and placebo in allowing the rats to avoid
being paralyzed and in reducing the subsequent damage to the spinal cord
(additionally, when both were given together, there was less scarring, collagen
formation and damaged nerve fibers).
When the sensory nerve signals
(somatosensory-evoked potentials) and motor function of the hind legs of rats
were evaluated after a spinal cord injury that was followed by a therapy, DMSO
given intraperitoneally 1 hour after therapy, 14 days later, produced
significantly better results than methylprednisone (a steroid) or naloxone.
Note: numerous
studies have found DMSO
somatosensory-evoked potentials and that their presence correlates
with an improved prognosis and an eventual full recovery.
Another dog study where blunt trauma was applied to the spinal cord at T12 found that neurological surgery and IV DMSO (one hour after injury, and once daily for the first two post operative days) resulted in the recovery of walking, running ability, cortical-evoked potentials, and histological improvements (less cavitation, meningeal hyperplasia, and necrosis of the cord), whereas dexamethasone (a steroid), reserpine and hypertonic dextrose did not offer any improvements.
When neurons from guinea pig spinal cords were cut, DMSO was shown to repair neuronal membranes, and enhance the ability of their axons to reseal and regain their membrane potential, possibly due to DMSO reducing inflammation and removing fluid cavitations from the spinal cord while increasing blood flow.
When the blood supply to the spinal cord was cut off in dogs, DMSO was shown to prevent ischemic myelopathy (damage) to the spinal cord and paralysis. In a rabbit study where its blood supply was cut off and then restored, DMSO protected the lumbar spinal cord from damage (assessed through electron microscopy), reduced the degree of oxidative damage, and protected the neurological motor function of the rabbits (assessed through the Tarlov score).
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Subscribed
DMSO and Protein Folding
Chemical chaperones are
small molecules that help proteins be folded into their correct configuration,
and hence can ensure protein stability or help the body eliminate misfolded
protein. Since many challenging diseases (particularly genetic ones) are a result
of misfolded or non-functional proteins, chemical chaperons offer a
potentially invaluable therapeutic strategy.
Note: I believe the physiologic
zeta potential has an important role in ensuring
the correct folding of proteins.
Some of the best-known chemical chaperones include glycerol, deuterated water, and DMSO (which is thought to be in part due to it creating a tighter packing around proteins and stabilizing their confirmation). DMSO, in turn, has shown promise in the following misfolding diseases:
•In nephrogenic diabetes insipidus (by rescuing mutant vasopressin V2 receptor proteins). Additionally, this study showed DMSO created a functional improvement of the cells.
•In cystic fibrosis by helping transport functional CTFR proteins to the cell membrane.
•In Machado-Joseph disease (a neurodegenerative disease characterized by discoordinated movement and eventually paralysis) by preventing aggregation of the ataxin protein and cell death caused by those aggregation.
•Increase the ability of impaired immune cells (due to them having defective HLA-DM) to present the antigens necessary to mount an immune response.
In Creutzfeldt-Jakob disease (a horrible and terminal condition), it reverts the mutant prion protein back to normal and prevents neurons from dying. DMSO has also been shown to prevent the aggregation of the scrapie protein (a related neurodegenerative condition).
Note: since many cancer causing proteins are misfolded proteins, it is thought that this may partly explain DMSO’s anticancer properties.
Amyloidosis
One of the most well-known protein misfolding conditions (which sadly is has also been linked to the COVID vaccines) is amyloidosis, a challenging to treat condition where misfolded proteins are produced in excess, clump together in the body, and gradually fill up organs, increasingly disrupting their function.
DMSO appears to have the ability to both dissolve amyloid aggregates and eliminate them from the body, and in all cases where it has been attempted, no adverse effects were observed (e.g., see this study). Those studies are as follows:
•Amyloidosis was induced in mice by repeatedly injecting them with casein and then treating them with DMSO. In mice that did not receive DMSO, their livers were loaded with amyloid, whereas in the treated mice, their livers were free of amyloid deposits, and broken up amyloid fibrils were found in their urine—demonstrating that DMSO dissolves the amyloid protein. Similar results were obtained in another study which concluded DMSO caused amyloid protein fragments to be eliminated in the urine.
•A human study found DMSO caused amyloid proteins to be eliminated in the urine.
•A case report discussed
a dog diagnosed with hypoalbuminemia, proteinuria, and renal amyloidosis. Two
years after the initiation of DMSO treatment, the 24 hour urinary protein
excretion returned to normal, while serum albumin concentrations increased to
within the normal range.
•A
case report discusses a woman with multiple myeloma and systemic
amyloidosis who took DMSO for 4 years and had her cutaneous lesions improve
(she, in turn, remained in good health 4 years after diagnosis—in comparison to
a median survival time of 14.7 months). In another case report, a
woman with pulmonary amyloidosis (due to multiple myeloma) received transdermal
DMSO for 8 weeks, and experienced a dramatic regression of her of her pulmonary
infiltrates (shown by x-ray) and a corresponding improvement or her arterial
blood gasses. Finally another case report also showed DMSO significantly benefitted
pulmonary amyloidosis.
•A retrospective study evaluated
10 patients who had developed secondary amyloidosis from rheumatoid arthritis,
Crohn's disease or Adult Still's disease (that were developing gastrointestinal
complications and early stage of renal dysfunction from their amyloidosis) who
took 3 daily doses of oral DMSO (in juice) after meals, dosed at 3–20 g/day in
a 33% solution. This improved the renal function in 5 out of 10 renal
amyloidosis patients (those given it earlier in the disease process), but did
not help those who already had severe or advanced renal dysfunction. In six
patients, specific improvements were seen in gastrointestinal amyloidosis, and
GI symptoms such as diarrhea, and protein-losing gastroenteropathy.
•In patients with amyloidosis secondary to leprosy, like the previous
study, DMSO
was found to improve those with moderate but not severe renal
failure (whereas the prior placebo gave no improvement).
•In
another study of patients with primary or secondary
amyloidosis, oral DMSO was improved the kidney function of those with secondary
amyloidosis and the authors emphasized that DMSO may significantly improve the
length of survival for patients with secondary amyloidosis. These results were
also seen in another study where
patients with secondary amyloidosis from rheumatoid arthritis, following 3-6
months of DMSO, had an improvement in their kidney function and a decrease in
the inflammatory activity of their rheumatoid arthritis.
•A girl with amyloidosis secondary to juvenile rheumatoid arthritis received topical DMSO and experienced a significant improvement in her gastrointestinal symptoms, kidney function (improved creatine clearance and a large decrease in her proteinuria), and heart (the amyloidosis had caused decreased left ventricular function).
•DMSO was given to patients with familial amyloidosis [FA], and was observed to cause urinary excretion of degraded amyloid proteins, with roughly half of the patients experiencing some degree of clinical improvement. In another report, two patients with FA causing peripheral neuropathy experienced significant improvement from DMSO.
•Another study of 13 patients who developed amyloidosis from a variety of causes found secondary amyloidosis was improved with DMSO.
•A small study of
patients with primary amyloidosis localized to the bladder (a challenging
condition) found the majority of patients benefitted from DMSO, that DMSO can
be a bladder saving measure, and that it can help resolve obstructions between
the bladder and ureters. This case report and this case report had
similar results.
•A study (reported
at a symposium) found DMSO successfully treated human amyloidosis secondary to
rheumatoid arthritis (which was also further
discussed at the symposium).
Many other studies also exist in this area. For example:
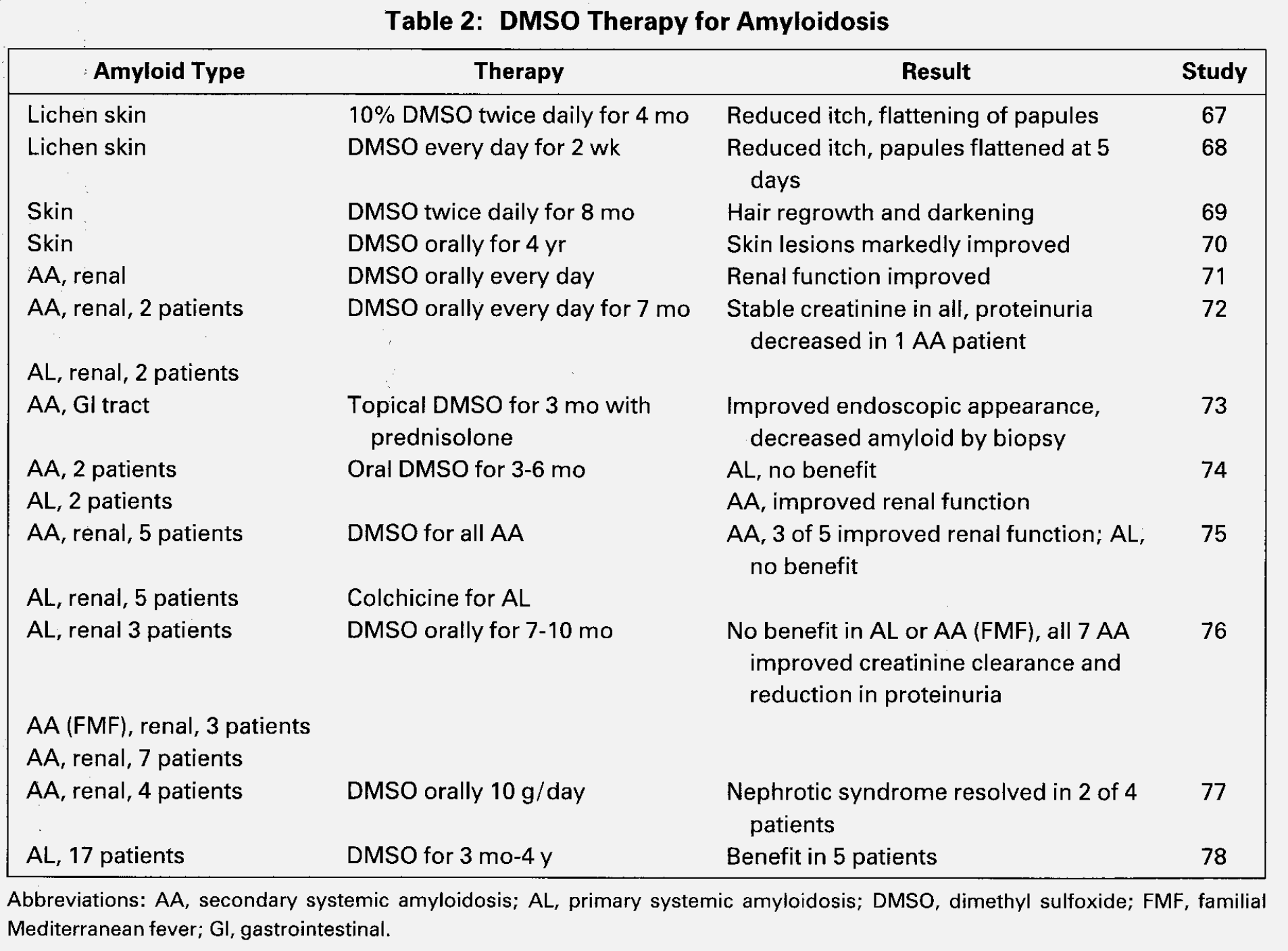
Links to above studies: 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77. 78-[only a citation]
Lastly, Niemann–Pick disease (a fatal and incurable condition) results from a genetic defect which causes metabolites to excessively accumulate with cells because the proteins that should remove them don’t function properly. This disease frequently leads to severe complications such as severe neurological impairment, gradual loss of cognitive function, and organ swelling. In this, this, this, this, and this study, DMSO increased the cell’s ability to remove those metabolites, and according to this paper, oral DMSO clinically improved Niemann–Pick type C patients (e.g., there was a reduction in hepatosplenomegaly and seizure frequency).
Cognitive Impairment and Dementia
Since many neurological
disorders are linked to poor blood flow to the brain, previous traumas (e.g.,
concussions or microstrokes), the accumulation of misfolded proteins (e.g.,
this characterizes Alzheimer’s disease), or an autoimmune process (something
DMSO also helps greatly with), it stands to reason that many cognitive
disorders would respond to DMSO.
In turn, this is what we find, and that much in the same way DMSO reverses many
other complications of aging (e.g., skin issue, hair loss, poor organ function)
IV DMSO is one of the most effective anti-aging therapies for the brain (along
with ultraviolet
blood irradiation or improving
the physiologic zeta potential). Likewise, IV DMSO is one
of the only therapies I know of which can help challenging neurological
diseases Parkinson’s or ALS (where in both cases, while not curative, typically
halts the progression of the disease). In turn, I periodically come across
anecdotes of DMSO consuming centenarians who have no cognitive impairment
despite their age.
Note: later in the series, I will also
discuss how DMSO helps multiple sclerosis.
The animal research in this field is as follows:
•A study surgically modified rat carotid arteries to significantly reduce the amount of blood going to their brain. After 3 months, it was found that DMSO prevented both the neuronal damage and the significant loss of spatial memory and learning that otherwise resulted from that chronic loss of cerebral blood flow.
•In a similar study, rats 14 weeks old were subjected to either permanent bilateral carotid artery occlusion or sham occlusion (mimicking the chronic vascular impairments many experience with increasing age) and then tested the rats for visuospatial memory function. After 14 weeks, four rats who had shown persistent and severe memory impairment received DMSO and FDP for 7 days, which improved their memory by 54%, almost reaching the cognitive function of the controls. Unfortunately, this improvement was partially lost once DMSO-FDP were discontinued.
•In mice genetically engineered to have Alzheimer’s disease [AD], DMSO has been shown to increase neuronal density in the hippocampus (a brain region vulnerable to AD) and enhance their spatial memory and smell (while decreasing their anxiety).
Note: DMSO has also been shown to greatly delay (48-98%) the paralysis caused by amyloid beta in C. elegans (one of the most popular organisms for aging research) and to extend the lifespan of C. elegans by 23.0-24.4%. The researchers attributed this delay in paralysis to DMSO modulating neurotransmission (e.g., DMSO is an acetylcholine esterase inhibitor, a therapeutic strategy also used to treat Alzheimer’s disease).
•Lurcher mice are used to study olivary and cerebellar disorders because their Purkinje cells can’t survive (e.g., by 30 days of age their walking is grossly abnormal). When these mice received DMSO, it prevented the age-related deterioration of certain cognitive functions (e.g., memory and spatial learning abilities)
While human research has also been conducted, I could not locate any of it online. Those studies are as follows:
•In this study 18 patients with probable Alzheimer’s were treated with DMSO and tested regularly for nine months, with great improvements being noted after only three months of treatment, and becoming especially noticeable after six months of treatment. Areas of improvement included memory, concentration, and communication alongside a significant decrease of disorientation in time and space.
•Another study evaluated 104 elderly adults with organic brain disease due to cerebrovascular diseases (e.g., a previous stroke, cerebral embolism or a hardening of the arteries of the brain), a previous head injury, senility, or degenerative disease (e.g., Parkinson’s, hyperthyroidism or epilepsy). They received two DMSO mixes, Merinex (DMSO with amino acids) and Ipran (DMSO with vasoactive substances), typically alternating between the two, and for the majority of the time as an injection, and a minority of the time orally (with the fastest results occurred if both routes were used simultaneously), all of which resulted in remarkable improvements. To quote the author:
The DMSO aminoacid therapy is undoubtedly valuable in the treatment of numerous organic cerebral diseases. At the same time, thanks to the improved cerebral blood irrigation achieved by DMSO used in combination with vasoactive substances, a highly favorable effect on the psychic and somatic functions of senile patients was achieved.
•A Chilean study evaluated 100 patients with cerebrovascular diseases (e.g., a previous stroke, cerebral embolism, or a hardening of the arteries of the brain), many of whom were senile, that received DMSO orally and through intramuscular injections over the course of 50 days. There it was noted that their coronary heart disease (i.e., atherosclerosis) and high blood pressure had a good improvement in 74.35% of DMSO recipients, a fair response in 21.77%, and no response for 3.88%. The neurologists overseeing these patients remarked that:
“Recovery from the general symptoms was positive; there were favorable changes which were reflected in a feeling of well being, the recovery of agility, changes of mood from depressed to gay, improvement of sleeping, and clearer speech. As regards the ‘focal’ results, accelerated recovery from hemiplegia and hemiparesia was registered. A speedier recovery of speech in cases of defined or indicated aphasia took place.”
Psychiatric Conditions
Another one of my favorite therapies, ultraviolet blood irradiation, essentially works by increasing circulation throughout the body, decreasing inflammation, and reawakening cells that have entered a dormant state (before they die). In turn, since these issues underlies so many different disease processes, a vast body of literature demonstrates it’s remarkable efficacy for a wide range of conditions, including psychiatric ones. As DMSO also essentially does these three things, some data has accumulated on its value in psychiatry.
In a study at a Peruvian psychiatric hospital, 42 patients (25 schizophrenics, 4 manic depressive psychotics, 4 alcoholic psychotics, 4 compulsive-obsessive neurotics and 5 patients with severe anxiety) were taken off all their medications then given 2-5 intramuscular injections each day (with more given to the most psychotic patients) and compared to 16 controls receiving standard care.
Of the schizophrenic, all 14 of the acute cases experienced a rapid and dramatic improvement (particularly in their agitation—especially for the catatonic-paranoid patients), with all being discharged within 45 days (three having a complete recovery 15 days after admission) and not having a recurrence. To quote one of them:
“I have been out of my mind. I don’t know what happened to me. I wonder what my children are going to say.”
Of the 11 chronic schizophrenics, 4 periodically needed hospitalization and had a complete remission following DMSO (allowing them to be discharged much faster than normal), and in those who later relapsed, there was again a positive response to DMSO. The remaining 7 were more severe cases (e.g., they had been hospitalized for over 6 years and failed years of therapies) and experienced an improvement from DMSO, but it was not enough to leave the hospital.
Note: results like this (I’ve seen similar ones with other therapies as well) lead me to believe that the existing understanding of schizophrenia is extremely incomplete. To further support that contention, this author also shared a case of a severely delusional paranoid schitzophrenic responding to DMSO.
The 4 manic-depressive psychotics (who were in the manic phase, averaging 15 days of psychomotor agitation) rapidly calmed down and lost their mania after DMSO (with their recovery being much faster than what they’d previously experienced from conventional therapy).
The 4 alcoholic psychotics
(2 with hallucinations and 2 with delirium tremens) had previously been
hospitalized for these issues. They rapidly responded to DMSO, with
restlessness improving in the first few days while the hallucinations took
longer.
The remaining patients (obsessive-compulsive neurosis and severe anxiety) also
had a good response to DMSO (e.g., they were calmer, ideas did not upset them
as before, they were able to act in a more spontaneous way, and they were able
to overcome their obsessive compulsions).
Developmental Disabilities
One of the most remarkable effects of DMSO is its effects on developmental disabilities. For example, at a hearing Congress convened to (unsuccessfully) pressure the FDA to end its embargo on DMSO, testimony was given of a child with Down’s Syndrome (classically considered incurable) having a miraculous response to DMSO.
![]()
1980 Congressional DMSO Hearing
21.9MB ∙ PDF file
There, Melody Clark, was discussed, who at 11 months (unable to stand or walk, had protruding tongue and all the classic Down Syndrome symptoms) was started on DMSO. She improved and at eight years of age, was able to walk, run, talk, read, and spell almost normally—something her teachers had never seen in another child with Down’s Syndrome. Specifically, she functioned at a second-grade level (with verbal competency and excelling in arithmetic), could engage in normal physical activities, and was very socially minded (allowing her to be quite popular with her peers).
In short, she transitioned from a vegetative existence (e.g., initially she couldn’t stand and her eyes were constantly out of focus) to having a minor developmental disability.
Note: Melody’ dentist provided testimony that her mouth and palate had largely normalized (another common issue in Down’s Syndrome), something he had never seen occur in this patient population.
Two other similar cases have also been reported:
•At 10 months of age, Bronwyn Nash (who had Down’s Syndrome) was frail and unable to gain weight, so her mother started her on DMSO. She began gaining weight and developed an increased awareness of the people and objects around her and then started reaching out to touch things. At 18 months, she was able to stand up, and then became able to get into her mother’s cupboards, started to feed herself, and held her water glass well. At the time a health journalist visited her at 28 months of age, she was an alert, cheerful little girl much enjoyed and well loved by her family and improving steadily.
•At 14, Billy King could walk and feed himself but had the mental capacity of a ten month old. He then began drinking milk with DMSO each morning, and two years later, had the mental capacity of a seven year old and began losing the characteristic Down’s "Syndrome appearance.
Before treatment, 1 year into treatment and 2 years into treatment.
He continued to improve and was eventually able to hold a job in a Portland bookstore.
Note: another account of Billy King’s story has a different chronology (e.g., he started DMSO at 8 not 14, and also took the amino acid formula).
Research in turn exists to support these unbelievable anecdotes.
•In Oregon, 67 moderately or severely mentally disabled children (aged 4-17) with Down’s Syndrome were randomized to receive a high or low DMSO dose and then were compared to 23 similar children whose parents did not want them to receive an experimental drug. No side effects occurred and a dose dependent improvement was observed:
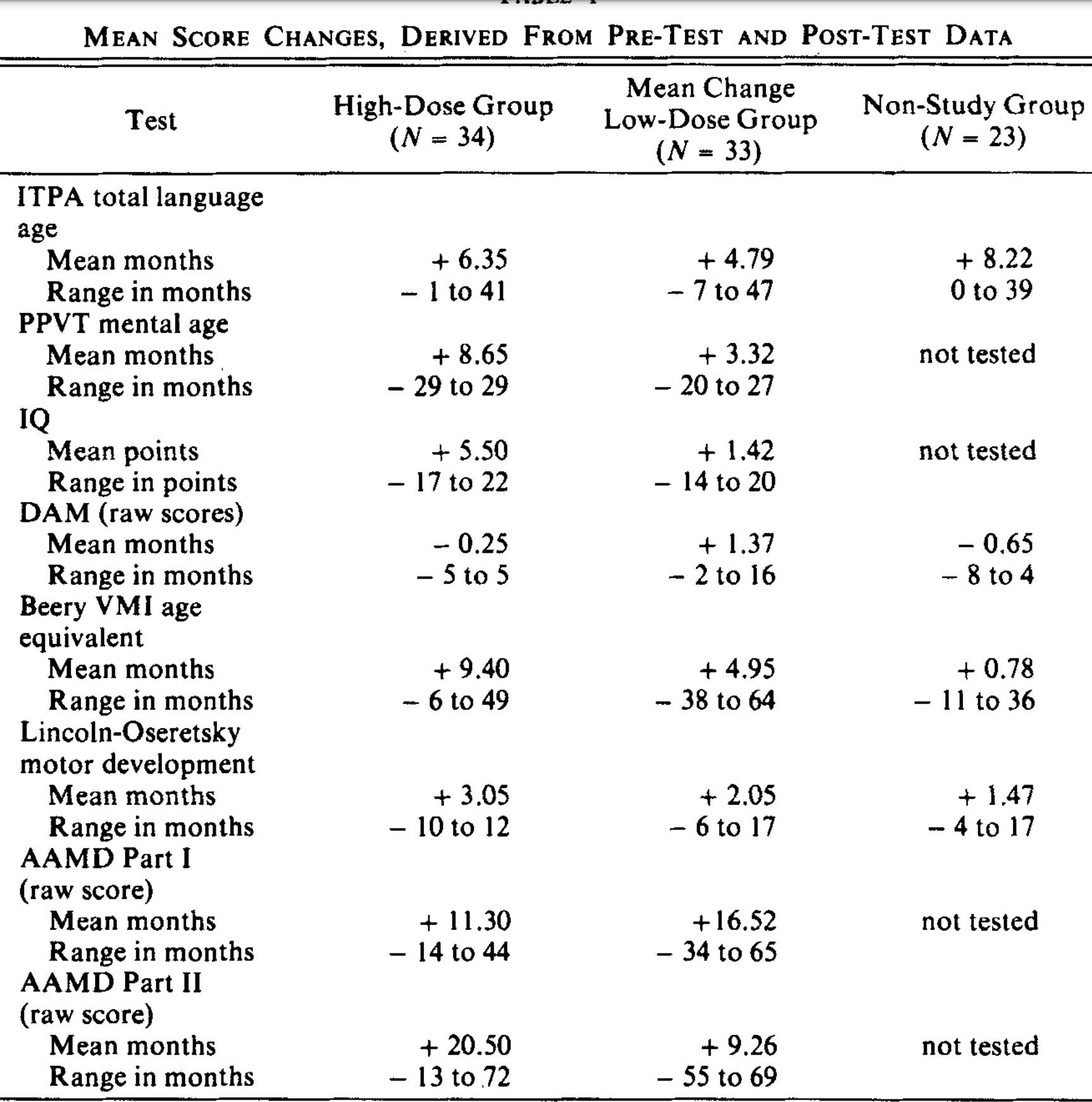
In Chile, 55 children with severe mental disability caused by Down’s syndrome (the oldest being 14) were given DMSO and amino acids by intramuscular injection or served as controls. The vials for injection consisted of DMSO along with gamma aminobutyric acid (GABA), gamma amino beta hydroxybutyric acid (GABOB), and acetyl glutamine (with lower doses given to those under 3 1⁄2 years of age). The children’s development was then evaluated with Gessel scores and a massive improvement was seen in the DMSO group:
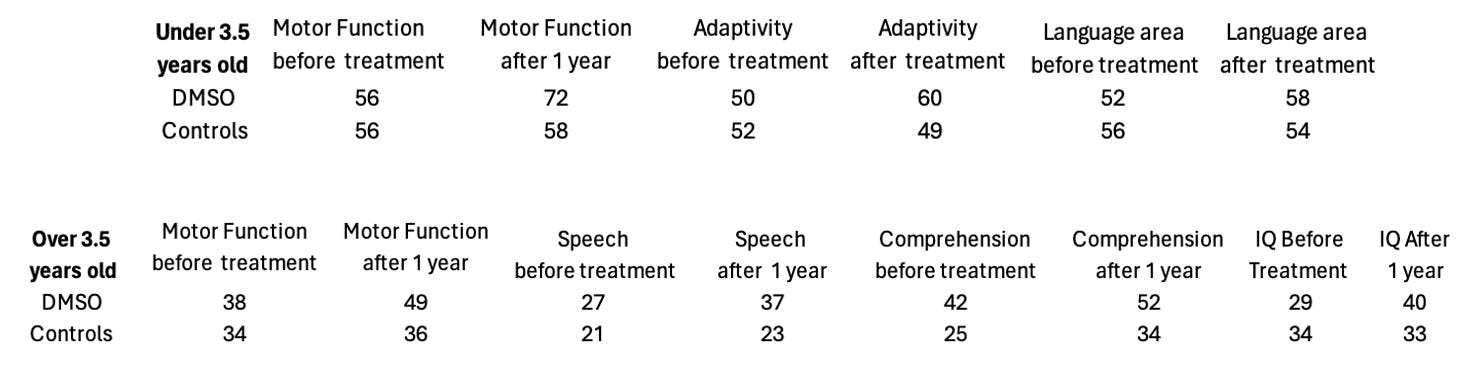
Note: this study (and the additional improvements that occurred) can be viewed here and here.
In Argentina, 13 mentally disabled children (5 severe cases, 4 moderate cases, and 4 mild ones), who did not have Down’s Syndrome, received a DMSO amino acid mixture (known as Merinex) three times a week by injection for 180 days (with periodic 15 day periods where the amino acids without DMSO were administered orally)
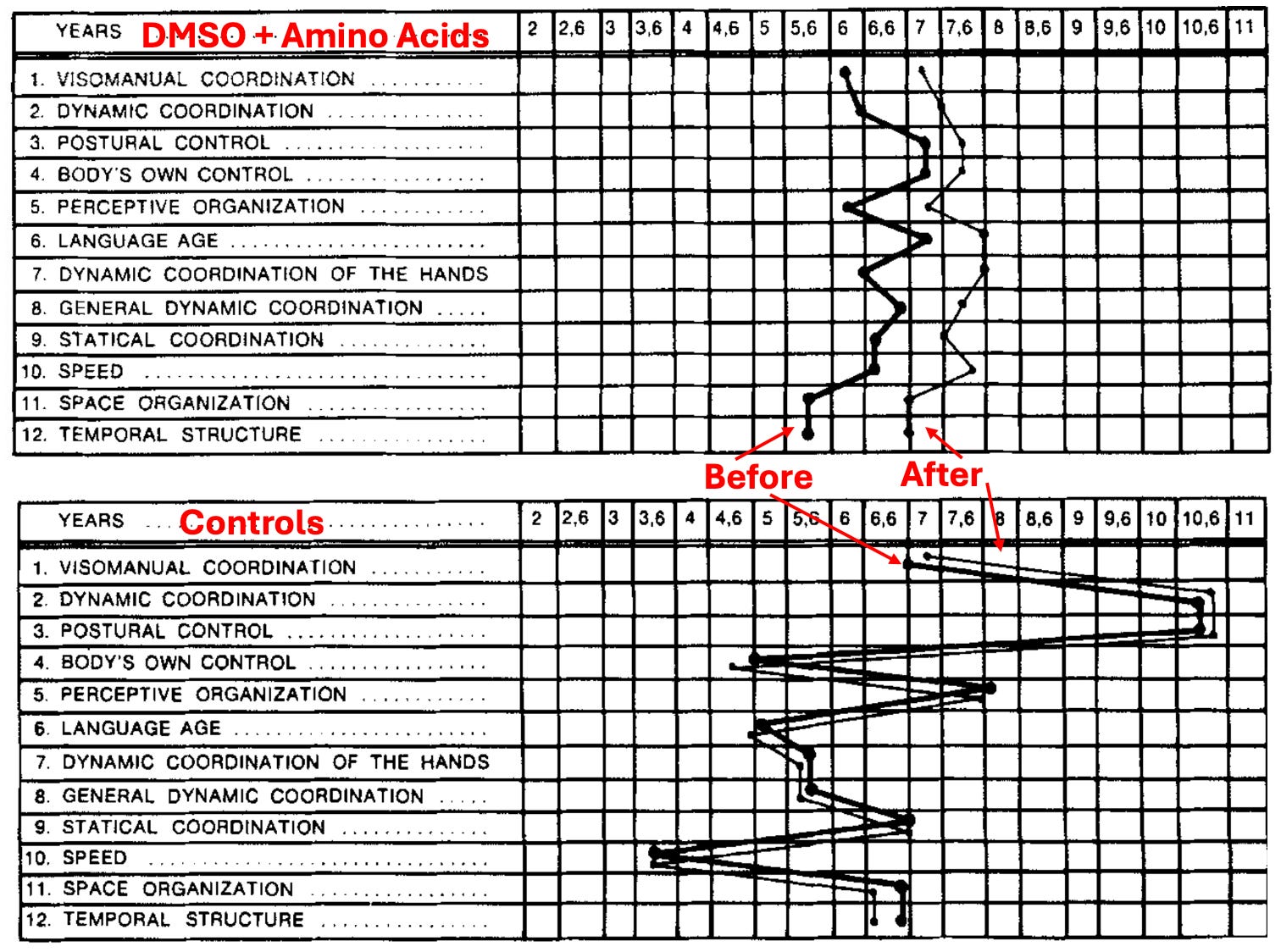
Note: other authors have reported young patients (and older ones) with learning difficulties, low intelligence, ADHD, anxiety disorders, epilepsy, nervousness, dyscalculia, dyslexia, exhaustion, and concentration problems all benefit from this protocol. Additionally, some have argued adding galactose to it enhances its efficacy.
In a 1969 study, 44 severely developmentally delayed children received the DMSO amino acid mix, with many experiencing a heightened capacity for learning in them in a relatively short time and over 70% having favorable responses such as a “increase of the IQ, an evident and accelerated progress in basic achievements, an overall improvement of intellectual capacity, evident progress in reading, writing, and mathematics, better coordination of movements and improved manual skill, and a decrease of behavioral problems," along with gaining better psychomotor control, no longer having anger for no reason, a general reduction of irritability, and a lessening of disobedience.
Another 1969 study gave the DMSO amino acid mixture for six months to 30 learning disabled children with language disorders (who did not have an accompanying neurological illness) and compared them to 20 controls, and observed it resulted in:
1. Disappearance of mental
lethargy.
2. Evidence of sensorial reactions.
3. Disappearance of automatic movements.
4. Disappearance of inertia, passivity, and negativity.
5. Growing interest and initiative in tasks and activities.
6. Improvement of the physiognomic expression and of the spoken language.
7. Lucid activity, group contact, and disappearance of unprovoked
aggressiveness.
8. Losing shyness and developing self-esteem.
9. Successful training to carry out chores, to do shopping, to eat, and to
dress without help, etc.
10. Learning to read and to write and to do homework.
Lastly, one author reported on an Argentinian study (I could not find) conducted by this physician. where 18 children with Down’s syndrome received DMSO and amino acids and were compared to 91 controls, and to quote the author this resulted in:
a tendency towards accelerated maturity in the children treated, with marked progress in language integration; this could be established in statistically significant degrees in the children treated
Note: a different book authored by the leading DMSO researcher reported that veterinarian Jack Metcalf had found horses developmentally disabled at birth (to the point they can’t nurse) once given IV DMSO three times daily regain the ability to nurse and that DMSO accelerates their overall development.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Subscribed
DMSO in Context
Because DMSO had the fortune to be discovered at a time when there was still an unbridled enthusiasm within the scientific community to investigate an unorthodox idea (something which has largely disappeared now because career scientists are so dependent upon not rocking the boat to ensure a lifetime supply of research grants) and it fell into the right people’s lap (exceptionally talented, ethical and driven physicians who’d earned the support of their superiors) the scientific community rallied behind it and published thousands of papers on DMSO.
Nonetheless, the FDA was still able to squelch it, and all of the research behind it (along with all the animals that were sacrificed to attain it) have been consigned to the dustbins of history. In the case of DMSO, this is particularly tragic because of how much suffering (and economic cost) many of the disorders discussed here create and the fact that decades of research and billions of research dollars have brought us no closer to solving them.
I thus made the decision to present this in a neutral tone and do my best to accurately present that science behind DMSO (which has required hundreds of hours of work) so I could give DMSO the best chance of flourishing now and helping those it could help—but in truth—words cannot begin to express my disdain over how DMSO was treated or the human cost of the callous bureaucratic dictates which have kept it from being adopted within the medical system (a sentiment I believe will be shared by many of you). For example, this is what Pierre Kory said after I asked him to review this article:
In the over 15 years I spent running ICU’s managing many kinds of brain injuries, strokes and bleeds, it both infuriates and saddens me to know of an intervention that could’ve helped so many of the hundreds of devastating neurological illnesses that I valiantly and often largely unsuccessfully tried to reverse to health. The therapeutic strategies that I had to rely on like tPa were often quite limited in impact or introduced major risks to the patient.
Note: the reason this project has taken so long is because even here, I only touched the tip of the iceberg, and there are still many other paradigm shifting uses for DMSO (e.g., it is a safe and effective painkiller, it treats both acute musculoskeletal injuries and chronic ones creating significant physical impairment, and it provides a way to treat many other challenging conditions that still do not have an effective therapy within the standard of care). In turn my hope is provide the rest of the DMSO in the near future.
As so much has been forgotten about DMSO, few are aware of its intravenous applications (even its proponents). In the final part of this article, I will discuss everything we know on the subject (e.g., where to procure it, what supplies to use, how to dose it) and the non-IV protocols we’ve used for strokes (since IV DMSO was often not feasible in those situations) and other traumatic injuries both at the time of injury and afterward for recovery (e.g., IV DMSO is one of the best options for stroke rehabilitation).
Procuring DMSO:
When trying to attain DMSO, the primary goal is to obtain the highest purity possible and for it to be stored in a container that DMSO will not absorb the contents of. Because of this, I generally advise people to get the highest purity product possible. For years, I used the brand on the left, but more recently, a newer one came out that also works well:

Both of these can be purchased online by searching “DMSO” (e.g., on Amazon). Additionally, the pioneer of DMSO developed his own line of high purity DMSO (which can be purchased here and more importantly has human beings on the other end who understand a lot about the subject).
Note: for much of DMSO’s history, because it was not available as a medical product, people often used industrial grades which had contaminants present—but to my knowledge no one ran into significant issues from doing that, so while I strongly advise getting a pure product, I don’t actually know how vital it is to do.
For intravenous DMSO, the major consideration is to avoid having the standard contaminants which can make people ill (e.g., microbial contaminants). Since DMSO inhibits the growth of bacteria, this risk is lower in pure solutions, and I’ve come across numerous authors (e.g., this one) who suggested just getting pure DMSO and then running it through a sterile (polytetrafluorethylene or polyamide) 200nm or smaller nanofilter before introducing it to the body, and I’ve never heard of an issue arising from that. Nonetheless, I (and everyone I know) will only use a sterile DMSO product for IV or IM use, and there are essentially 3 options for how to procure that:
•The first is to get the 50% DMSO solution (RIMSO-50) which the FDA approved for intravesical (within the bladder) use. Of the options, this is typically the most costly.
•The second is to get a pure cellular preservative. Many people I know prefer Cryoserv (since it works well and is cheaper).
•The third is to order it from a compounding pharmacy (which can be the cheapest option).
Note: despite the evidence presented here, there is currently no FDA-approved use for intravenous DMSO (besides using it in combination with something like Onyx).
Using DMSO:
Prior to
using DMSO, it is ideal to verify you are not one of the 1/2000 people who is allergic
to it (which may not be possible in an emergency situation) and to have
it on hand for when you might need it. The easiest way to test for
an allergy is to apply it to the skin and see if anything more than temporary
itching or redness (common reactions to DMSO) occur (e.g., do you get hives or
a rash somewhere else).
Additionally, it is generally advised to avoid
going over 70% (because this can increase irritation) but at the same
time, higher ones can also be used (especially if temporary skin irritation is
not the primary concern).
Note: from a provider standpoint, this is another argument for having the basic supplies for an anaphylactic reaction on hand.
In these situations, DMSO is normally applied topically or taken orally (since it's unlikely an IV set-up will be available) and sometimes injected intramuscularly..
My somewhat unique approach (which seems to work but I simply don’t have enough data on) is to apply DMSO topically to the artery that feeds the area of the stroke.
Most commonly this is either the left or right carotid (the major artery you can feel on the front of your neck). In most cases, strokes in the arteries the carotids feed (e.g., the MCA) tend to affect the opposite side of the body. So if there is a right sided facial droop or numbness and weakness on the right side, that tells me there is an issue in the left MCA, and DMSO needs to be applied to the L. carotid artery. If possible when applying DMSO, I also have the person lie down so that when applying DMSO the gravity will pull it to the artery below, but that is often not practical (and I am still not sure how much it matters).
Additionally, strokes can often occur in other parts of the brain (e.g., those fed by a vertebral artery), so exactly which artery I tell them to prioritize depends on the situation. That said, applying it anywhere on the skin will still get it into the body, and I often also instruct people to apply it to both carotids.
Note: people I am very close to would have likely had a lifetime of disability if I had not been able to get them to use DMSO once their stroke started so I feel very strongly about this concept being known.
Finally, many of these approaches can also be used to rehabilitate an old stroke or spinal cord injury.
DMSO Compatible Materials
One of the major challenges early investigators had was determining which IV materials could transport DMSO without any of it being dissolved or leached by DMSO (e.g., this was an issue one group of unfamiliar investigators ran into).
For example, arterial catheters made of polycarbonate, polystyrene, styrene-acrylonitrile, and polyvinyl chloride needed to be avoided because 100% DMSO could partly dissolve or chemically leach these products. DMSO was found safe to use with conventional or linear polyethylene, polyvinyl chloride, polypropylene, and teflon catheter systems, and products using these plastics also included hubs in disposable needles.
One question that arose from these studies was the potential of DMSO to dissolve plastics. In the United States, most intravenous bags and tubing are made of polyvinyl chloride, which are safe to use with DMSO.
When in doubt, pour some DMSO on the plastic i.v. set in a beaker and leave for 12 hours. If solution becomes cloudy, use some other plastic system. DMSO should always look clear and colorless.
Sadly, slightly conflicting
resources exist in this regard (e.g., this
website states DMSO is compatible with High-density polyethylene (HDPE),
Low-density polyethylene (LDPE), Nylon, Polyethylene terephthalate ethylene
(PETE), Polypropylene (PP), Polytetrafluoroethylene (PTFE) and not compatible
or partially compatible with Polyvinyl chloride, Polystyrene, Polycarbonate and
referenced this website,
this website and this
website.
The most direct testing I found came from this company which
stated that 80% or above DMSO affected PVC but lower concentrations
did not (something far above the IV dose). In turn, the crux of the matter is
that it’s unclear how if DMSO can be used with PVC (some people I know do it
without issue, and in the above passage the author both said it was and was not
compatible). My best guess is that all of this reflected the fact 100% DMSO was
often drawn up when preparing DMSO, but not during actual infusions. That said,
non-PVC IV systems do exist (e.g., this
company makes polypropylene IV bags—a DMSO compatible material
and this company makes polyolefin
bags—which according
to this patient also is DMSO compatible).
Note: polyolefin is a deliberately vague term for a more resistant family of plastics which includes polypropylene and polyethylene.
DMSO Dosing
One of the challenging aspects of DMSO is that different people respond to different doses. Fortunately, DMSO is very safe, so you are unlikely to run into serious issues from choosing the wrong dose. Nonetheless (at least until you have more experience with it), outside of emergencies, it is generally advisable to start with a low dose and work upwards.
Skin
The variability in dosing is especially true with skin applications. However, in a stroke situation, the potential side effects (a temporary rash from the skin being irritated by too high of a concentration) are of a priority than ensuring DMSO gets where it needs to. For this reason, I would advise using at least a 70% solution (as 50-70% is the minimum amount needed to reliably get it there), but I’ve also used 100% solutions without issues and had the patient benefit greatly from it.
Orally:
When taking DMSO orally, diluting it to 20% or less is typically advised so it’s more pleasant to drink. However, here, the focus is normally more on how much to consume in total rather than the specific concentration.
Note: DMSO can make one have to urinate for the next few hours, so individuals often find the best time to take it is at breakfast (rather than at night, or before a flight or meeting). Additionally, people often like to dilute it in juice (e.g., grape or tomato) or milk to eliminate DMSO’s bitter taste—but when doing this, it’s important not to let the DMSO settle to the bottom and surprise you at the end.
Suggested doses include:
•When an adult takes DMSO, start out at a low dose of about 3.5g in a glass of water, observe the effects, and then gradually raise it by 3.5g a day until you find the appropriate dose. This rate can be raised to 7g, but you want to be mindful not to hit a concentration that irritates the mouth or throat (which normally requires diluting it into multiple drinks once you’re taking over 10g a day.
•If you have significant issues (e.g., systemic joint pain) lower doses such as 0.05-0.1 g/kg can eventually be raised to 0.5-1g/kg.
•In the Oregon trial where DMSO was given to children with Down’s Syndrome, DMSO was dosed at either 0.01 g/kg body weight 5 times a week for 14 weeks or 0.10 g/ kg 5 times a week for 7 weeks, and then 0.50 g/kg for the remaining 7 weeks, with two 1 week breaks occurring where DMSO was not administered.
•Giving impaired children 0.5 g/kg by mouth, or 5ml of 5% DMSO (mixed with 5mg of gamma aminobutyric acid (GABA), 10mg of gamma amino beta hydroxybutyric acid (GABOB) and 10mg of acetyl glutamine)—which I believe was the Merinex formula given orally and by injection in the South American trials of developmentally disabled children.
Intramuscularly:
While this is a commonly used method (due to its ease and ability to get things inside the body or to a target area like an inflamed part of the spine), I have minimal experience with it, so I can only quote what others have reported.
•In the psychiatric study, 5ml of 50-80% DMSO was injected 2-3 times per day (with the most disturbed patients receiving up to 5 injections). In the more mild cases, or as patients improved, 50% rather than 80% was used.
•In the study of children with Down’s syndrome in Chile, they received 5ml 5% DMSO injections three times a week in a series of 20 injections with a break of 15 days between each series over a total treatment time of 180 days. For the children of less than 3½ years of age the dosage of the 5ml ampule of 5% DMSO (containing 5mg GABA, 10mg GABOB and mg l-acetylgltamine) was adjusted in relation to body weight—those that weighed less than 8 kg were administered 0.5 cc, those between 8 and 11 kg 1 cc, and those that weighed more than 11 kg 2 cc.
Intravenously:
A variety of different perspectives exist on the correct dosing for IV DMSO particularly given that the wholesale price keeps on going up (e.g., it’s now around 8-40 dollars a gram—which is quite frustrating given that DMSO costs virtually nothing to produce).
To quote the leading research in this field:
We now know that the optimal dose of DMSO in human patients sustaining a severe brain injury is 1 g/kg in a 28% solution mixed with 5% dextrose in water.
The minitrial using DMSO to treat intracerebral hemorrhage and ensuing arterial spasm by Mullan et al. indicates that a DMSO bolus or very fast drip at doses of 1 g/kg/8 h in a recommended 28% solution appears as a safe and effective regimen.
Also, hematuria from red cell osmotic hemolysis was seen in all patients only after the initial loading dose of DMSO. Hematuria was seen to stabilize after subsequent doses of DMSO.113 The loading DMSO dose has no other consequences other than lowering the hematocrit about 25%, a temporary reaction that paradoxically lowers blood viscosity and vascular resistance while increasing CBF.
Note: every reference I’ve found settles between 1-2g/kg (typically 1-1.5). In one detailed toxicity study. a researcher found giving 3 g/kg of DMSO (diluted to 40%) to rhesus monkeys for 9 days caused no detectable issues for 4 months after treatment.
We tend to use a much lower IV DMSO dose than any of the references I’ve come across (3-5g of 100% DMSO diluted in 100 ml of saline), but that is in part because we never used it in the acute setting where higher doses are needed (rather it is used for general neurological rehabilitation).
In the existing literature,
the issue they repeatedly ran into was that when a lower concentration was used
(e.g., 10%), it would trigger significant diuresis (urination), and there were
a few reported instances of hypernatremia or fluid overload occurring following
low concentration DMSO. Conversely, when a higher dose (above 30%), it would
sometimes trigger hemolysis of the weaker blood cells (likely from osmotic
stress) and bloody urination (which typically was inconsequential and only
happened initially).
Nonetheless, this caused many of the DMSO doctors to check the blood count of
their patients before treatment and during the initial phase of treatment), but
as long as kidney function and the hematocrit remained unchanged, they would
ignore it and continue treatment.
Some of the other dosing regimens I’ve come across are:
•Up to 20-80ml of 25% DMSO
given as an IV push 1-3 times a day (for conditions such as arthritis or
cancer, Parkinson’s or multiple sclerosis).
•500 ml of 10-20% DMSO (diluted in saline or 5% dextrose) dripped over 2-3
hours.
•A 50ml bolus of 28% DMSO mixed in 5% dextrose (this was the dose used in the
two studies of 10 patients with severe closed head injuries).
•DMSO 560 mg/kg in a 28% solution, FDP 200 mg/kg mixed in 5% dextrose twice
(this was the dose used in the 2002 clinical trial of 11 patients with ischemic
strokes).
•Daily IV pushes of 3gm of DMSO.
•If over 25ml of DMSO (27.5g) is to be taken at any one time, diluting it in 1000ml (rather than 500ml)
•For non-emergent cases, 1 g/kg, diluted in 500ml of fluid (typically saline or 5% dextrose), sometimes having micronutrients added in that is given daily for 5-10 days, followed by a 2 day break, before the treatment is again resumed. Typically, a half dose is given initially to observe the patient’s response.
Note: the clinical parameters of dosing IV DMSO (and the accompanying references) are discussed extensively in this book (which should probably be given to any doctor who is considering using it). Additionally, some patients find the drips are too fast (e.g., they cause nausea) and hence need to be slowed down (or do other measures like eating before the IV).
DMSO Providers
The people who I know
provide IV DMSO do not publicly advertise it, and likewise, except for a few
naturopaths, I have not found anyone online who does. Because of this, your
best option is one of the following:
•Find someone through word of mouth.
•Present the information in this article (or more likely in this series) to a doctor you have a good relationship with and see if
you can convince them to try it on you.
•Start with other routes of administration (e.g., orally).
•Contact these
people and ask them if they can point you towards anyone
[disclaimer, I have never corresponded with them—so I can’t say with certainty
this would work].
•Ask your local integrative medicine doctor if they have any suggestions, or,
if you don’t have one, look in a directory (ACAM has one of the best ones).
Note: older doctors are more likely to be familiar with IV DMSO, and
likewise, due to the politics around DMSO, those from Oregon (and to a lesser
extent Florida or Washington) will have a familiarity with it.
Conclusion
I put a lot of work into this article, and I sincerely appreciate your support which makes it all possible. I hope that you can help share the information here because it is crucial for people to know about. Thank you for allowing me to do this!
Click below to share this post!





364 Likes
·
364
62
Discussion about this post
Comments
Restacks